Page 1 of 14
RD2.1 | Patient Suitability Screening for Radiation, Contrast and Magnetic Fields — SDL Guide
Learning Objectives
- Take a structured pre-imaging clinical history covering allergies, renal function, pregnancy status and implanted devices.
- Screen a patient for suitability for ionising-radiation exposure, applying ALARA and AERB justification principles to pregnancy and paediatric requests.
- Screen a patient for safe administration of iodinated and gadolinium contrast agents, including renal-function, prior-reaction, metformin and thyroid checks.
- Screen a patient for safe exposure to the MRI magnetic field, identifying cardiac implantable electronic devices, cochlear implants, ferromagnetic foreign bodies and aneurysm clips.
- Integrate the three screening domains into a suitability decision for common clinical imaging requests, and document the decision appropriately.
INSTRUCTIONS
Choosing the right modality is only half of safe imaging; the other half is confirming that THIS patient can safely undergo it. Every imaging request carries one or more of three hazard exposures — ionising radiation, an injected contrast agent, or a powerful magnetic field — and each demands a specific, answerable clinical question before the patient enters the scanner. This module builds the screening discipline that the requesting clinician owns: a structured history of allergies, renal function, pregnancy and implanted devices that turns 'order the scan' into 'order the right scan, safely, for this patient.'
References
- Sutton's Textbook of Radiology, 6th edition, Chapter 1 (Physics and Safety of Medical Imaging) (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapters on Contrast Media and MRI Safety (textbook)
- Atomic Energy Regulatory Board (AERB) Safety Code for Diagnostic Radiology, India (guideline)
- ESUR Guidelines on Contrast Agents (European Society of Urogenital Radiology) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A junior doctor on a busy medical ward needs a contrast-enhanced CT abdomen to characterise a suspected pancreatic mass. She fills the request form, ticks 'with contrast,' and sends the patient down. What she did NOT check: the patient's eGFR is 24 mL/min/1.73 m², he is taking metformin, and he once developed facial swelling after a previous CT dye. Each of these is a screening failure that the radiology department cannot detect from the request form alone — and each can cause real harm: contrast-associated acute kidney injury, lactic acidosis, or a recurrent anaphylactoid reaction. The scanner is safe; the unscreened request is not. Patient suitability screening is the clinical step that stands between a correct modality choice and an avoidable adverse event, and it belongs to the doctor who orders the scan.
WHY THIS MATTERS
Competency RD2.1 requires you to obtain a relevant clinical history to select patients for imaging — to determine their suitability for radiation exposure, contrast administration, and exposure to magnetic fields, including allergies, renal function, pregnancy and implanted devices. This is not a paperwork exercise delegated to the radiographer; it is a clinical assessment that the requesting clinician is best placed to perform, because you hold the patient's history. A pregnant woman irradiated unnecessarily, a patient with an eGFR of 20 given iodinated contrast, or a patient with a non-conditional pacemaker sent into a 1.5-Tesla magnet — these are the preventable harms RD2.1 exists to stop. In examinations, in clinical postings, and in every real ward decision, the question 'is this patient suitable for this investigation?' is asked of the ordering doctor, and the structured screen you learn here is the defensible answer.
RECALL
Before reading further, bring to mind the foundations you have already met:
- Ionising vs non-ionising modalities: X-ray, fluoroscopy, CT and nuclear medicine deposit ionising radiation; ultrasound and MRI do not. This dichotomy drives which screen applies.
- Stochastic radiation risk: at diagnostic doses, carcinogenesis and hereditary effects are assumed to have no safe threshold — the basis of justifying every ionising request, especially in the young and the pregnant.
- eGFR and renal excretion: both iodinated and gadolinium contrast agents are cleared by the kidneys; impaired renal function is the central screening variable for contrast safety.
- MRI physics: a strong static magnetic field (typically 1.5–3 Tesla) plus radiofrequency pulses — the reason ferromagnetic and electronic implants are hazardous in the MRI environment.
- MRI is NOT contraindication-free: pacemakers, cochlear implants, ferromagnetic intra-ocular foreign bodies and certain aneurysm clips are recognised hazards.
If any of these feel unfamiliar, a quick review of the modality-principles SDL before continuing will make the screening logic below much clearer.
Why Pre-Imaging Screening Is a Clinician Responsibility, Not a Radiology Formality
Imaging safety begins at the moment a clinician decides to investigate, not at the scanner door. The requesting doctor holds the information that determines whether a patient is suitable for a given investigation — the allergy history, the renal function, the menstrual and pregnancy history, the list of implanted devices — and is therefore the person best placed, and professionally obliged, to screen before ordering. The radiology department applies a second safety check, but it cannot reconstruct a history it never receives; a request form that omits the eGFR, the pregnancy status, or the presence of a pacemaker exports an avoidable risk downstream. This is why patient suitability screening is framed as a clinical competency (RD2.1) rather than a departmental formality: the harms it prevents — fetal irradiation, contrast-associated kidney injury, an implant displaced in a magnetic field — are caused or averted at the point of ordering.
The screening task organises naturally around the three hazard exposures an imaging study can carry:
- Ionising radiation — relevant to X-ray, fluoroscopy, CT and nuclear medicine; the screen asks about pregnancy, age/radiosensitivity, cumulative prior dose, and whether the study is justified.
- Contrast agents — iodinated agents for CT/fluoroscopy and gadolinium agents for MRI; the screen asks about renal function, prior reactions, relevant medications (metformin) and thyroid status.
- The magnetic field — relevant to MRI; the screen asks about cardiac implantable electronic devices, cochlear implants, ferromagnetic foreign bodies and aneurysm clips.
A single request may invoke more than one domain — a contrast-enhanced CT engages both the radiation and the iodinated-contrast screens — so the safe habit is to run all three checks against every request and act on whichever apply.
The Structured Pre-Imaging History — What to Ask Before Any Investigation
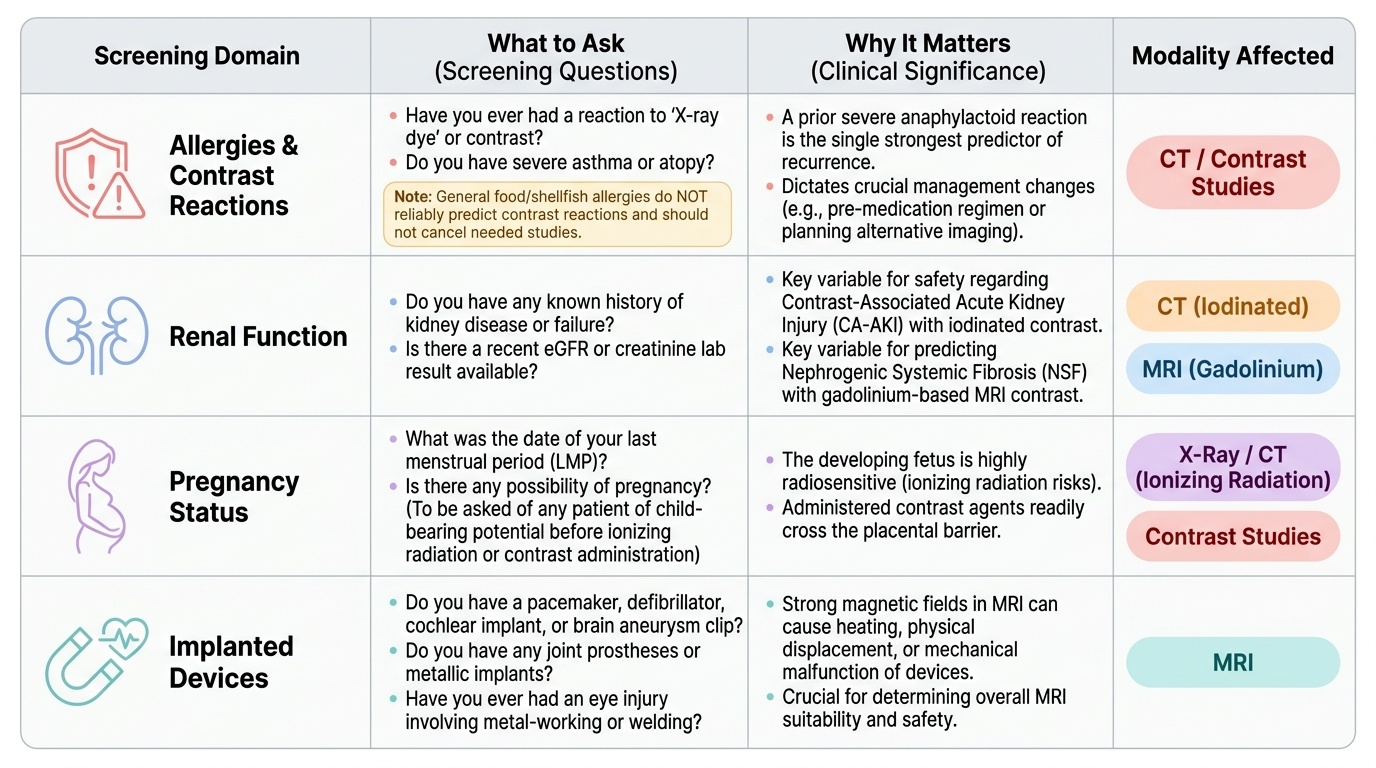
The most reliable way to make screening reproducible is to convert it into a structured history that asks the same four questions of every patient before any imaging request. Competency RD2.1 names these four domains explicitly — allergies, renal function, pregnancy, and implanted devices — and a clinician who asks them routinely will rarely be caught out by a hazard that surfaces only at the scanner. The discipline is to treat the four-domain history as a single mental checklist that runs automatically, in the same way a pre-prescription history runs through allergies and interactions; it takes under a minute and converts most preventable imaging harms into anticipated, managed decisions. What follows is the canonical set, with the clinical reason each item is asked and the modality it most affects.
- Allergies and prior contrast reactions: ask specifically about previous reactions to 'X-ray dye' or contrast, and about severe atopy/asthma. A prior severe (anaphylactoid) reaction to iodinated contrast is the single most important allergy item, because it predicts recurrence and changes management (pre-medication or alternative imaging). General food/iodine/shellfish 'allergy' is NOT a reliable predictor of contrast reaction and should not by itself cancel a needed study.
- Renal function (eGFR/creatinine): ask about known kidney disease, and obtain a recent eGFR before contrast. Renal impairment is the central variable for both iodinated (contrast-associated AKI) and gadolinium (nephrogenic systemic fibrosis) safety.
- Pregnancy status: ask the date of the last menstrual period and the possibility of pregnancy in any person of child-bearing potential before an ionising study or before giving contrast. The fetus is the most radiosensitive 'organ,' and contrast crosses the placenta.
- Implanted devices and metallic foreign bodies: ask about pacemakers/defibrillators, cochlear implants, aneurysm clips, joint and other prostheses, and any history of metal-working eye injury. These are decisive for MRI suitability.
Provided image
Screening for Radiation Exposure — Justification, Pregnancy and Paediatric Radiosensitivity
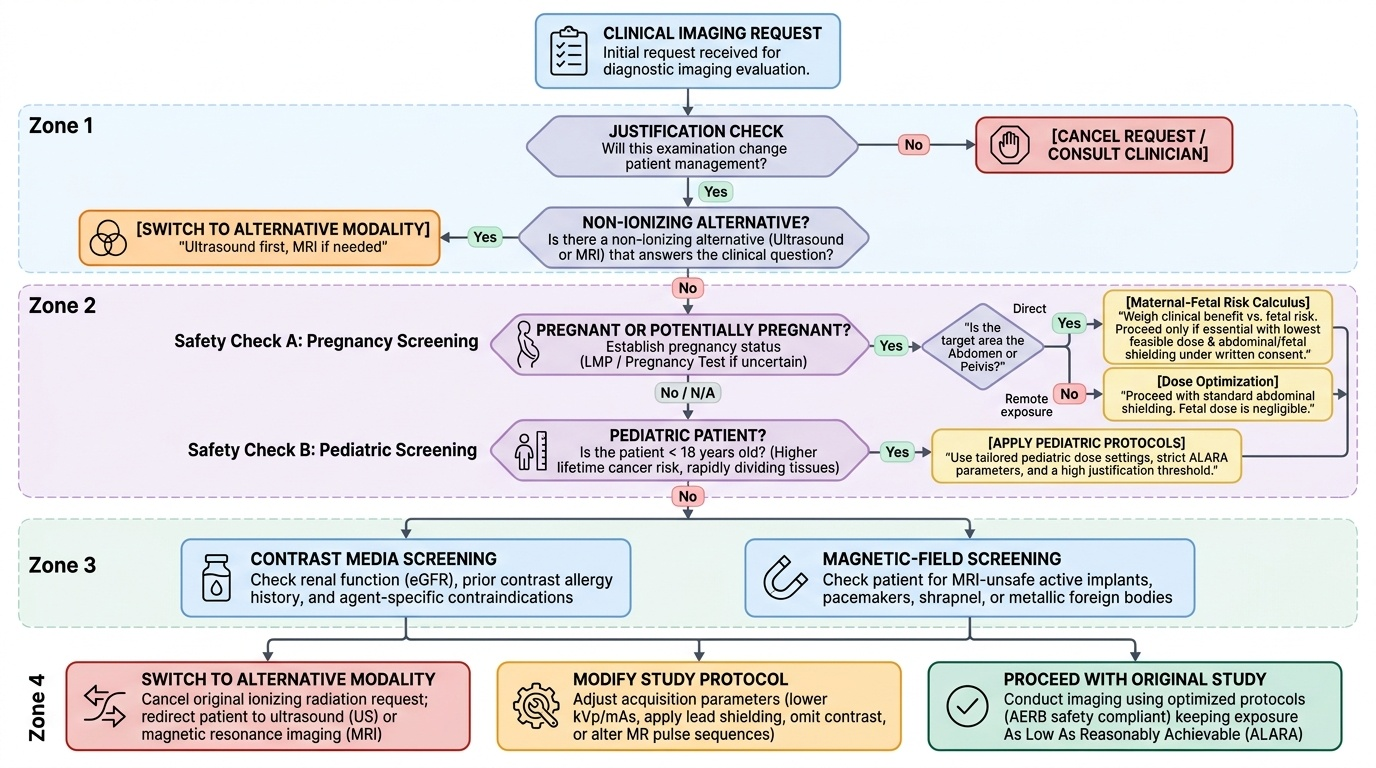
Screening a patient for ionising-radiation exposure rests on the principle that radiation carries a stochastic risk — principally carcinogenesis and hereditary effects — for which no safe threshold is assumed, so the dose-to-benefit calculus must be made deliberately for every request. The first and most important screening question is therefore one of justification: will this examination change management, and is there a non-ionising alternative (ultrasound or MRI) that answers the same clinical question? This is the core of the ALARA principle (As Low As Reasonably Achievable) and is mandated for Indian facilities by the Atomic Energy Regulatory Board (AERB), the statutory radiation regulator under the Atomic Energy Act 1962 — not the US NRC or the international advisory body ICRP. Two patient groups demand heightened screening because their radiosensitivity is greater.
- Pregnant patients: the fetus is the most radiosensitive subject, particularly during organogenesis. Pregnancy status must be established (last menstrual period; pregnancy test if uncertain) before any ionising study of the abdomen/pelvis or before contrast. If an ionising study is genuinely necessary for the mother, it may proceed with the lowest feasible dose and shielding, after weighing maternal benefit against the small theoretical fetal risk — but a non-ionising alternative (ultrasound first, MRI if needed) is preferred whenever it answers the question. Imaging remote from the fetus (e.g. a chest X-ray with abdominal shielding) delivers a negligible fetal dose and should not be withheld when clinically needed.
- Paediatric patients: children have more radiosensitive, rapidly dividing tissues and a longer lifetime over which a radiation-induced cancer can manifest, so the threshold to use ionising imaging is higher and child-size (dose-reduced) protocols are used. Ultrasound is the preferred first modality for many paediatric abdominal and hip problems precisely to avoid radiation.
The practical protection levers — minimise time, maximise distance (inverse-square law), and apply shielding — apply once a justified ionising study proceeds, alongside dose-optimised technique. The screening decision, however, is made before any of this: is the ionising study justified for this particular patient, and is a safer modality available?
Provided image
SELF-CHECK
A 25-year-old woman with a possible 6-week pregnancy presents with right-upper-quadrant pain and a clinical suspicion of gallstones. The intern requests a CT abdomen. What is the most appropriate screening-driven action?
A. Proceed with the CT; gallstone disease justifies the radiation
B. Establish pregnancy status and choose ultrasound first, as it answers the biliary question without ionising radiation
C. Proceed with CT but without contrast to reduce risk
D. Defer all imaging until after delivery
Reveal Answer
Answer: B. Establish pregnancy status and choose ultrasound first, as it answers the biliary question without ionising radiation
Screening identifies a possible pregnancy and a non-ionising alternative that answers the same clinical question. Ultrasound is the guideline first-line modality for biliary/gallstone assessment and carries no ionising radiation, making it the appropriate choice in pregnancy. CT (with or without contrast) exposes the fetus to ionising radiation and is not first-line for gallstones. Deferring all imaging is unsafe when a symptomatic diagnosis is needed and a safe modality exists.