Page 2 of 14
RD2.1 | Patient Suitability Screening for Radiation, Contrast and Magnetic Fields — SDL Guide (Part 2)
Screening for Contrast Administration — Iodinated and Gadolinium Agents
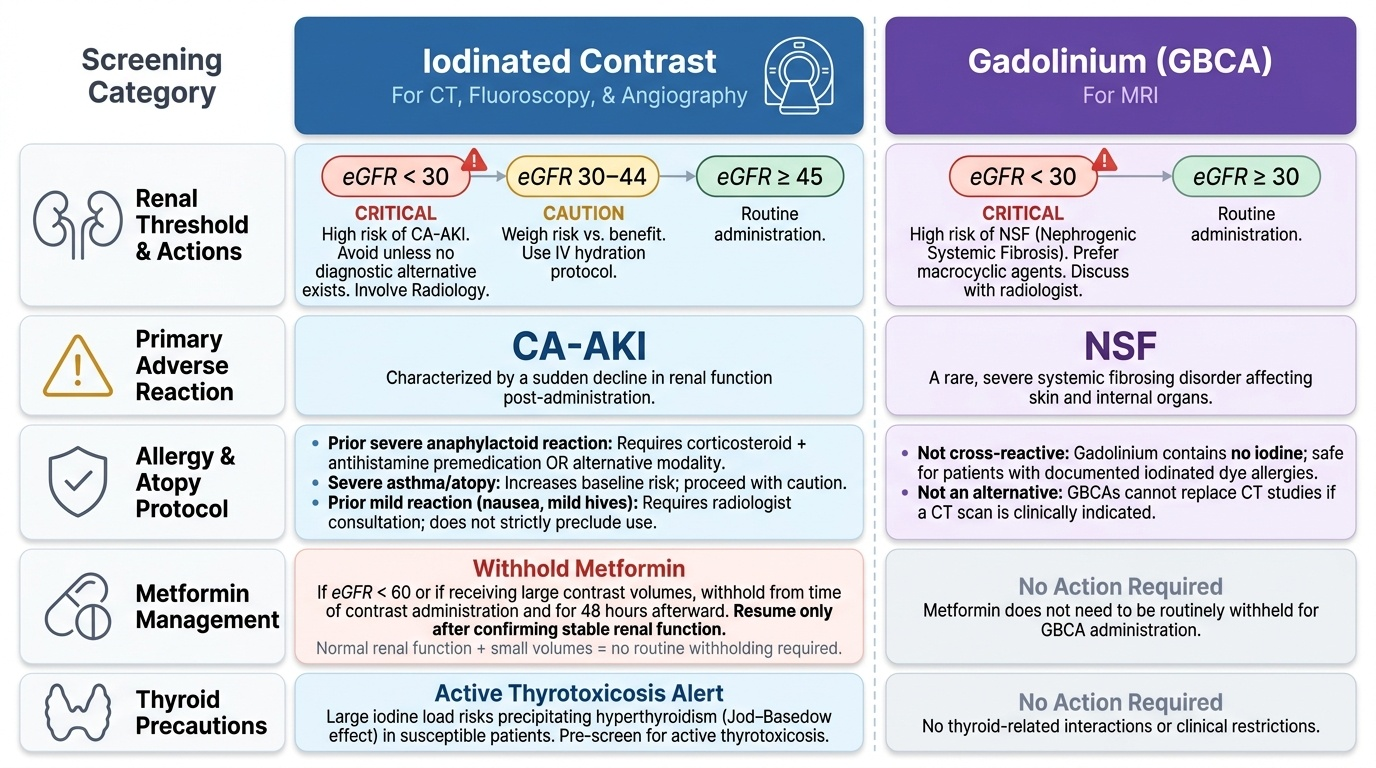
Contrast screening is a distinct, mandatory step whenever a study will use an injected agent, and the requesting clinician must complete it before ordering rather than leaving it to be discovered in the scanner suite. Two families of agents are used and they are NOT interchangeable: iodinated contrast for CT, fluoroscopy and angiography, and gadolinium-based contrast agents (GBCAs) for MRI; gadolinium contains no iodine and is therefore not an alternative for a patient who needs a CT but reacted to iodinated dye. Both families are cleared by the kidneys, which is why renal function is the pivotal screening variable for each, but the specific hazard each poses in renal impairment differs. The screen below should be run for every contrast request, and any positive answer triggers a discussion with the radiologist rather than an automatic cancellation.
- Iodinated contrast — renal function: the principal hazard is contrast-associated acute kidney injury (CA-AKI), with risk concentrated at eGFR <30 mL/min/1.73 m². At eGFR 30–44, proceed only after weighing need against risk with the radiology/nephrology team and using hydration; at eGFR <30, intravenous iodinated contrast is used only when no alternative achieves the diagnostic goal.
- Iodinated contrast — prior reaction and atopy: a previous severe anaphylactoid reaction requires premedication (corticosteroid + antihistamine) or an alternative study; severe asthma/atopy raises baseline risk. A prior mild reaction (nausea, urticaria) does not absolutely preclude contrast but warrants radiologist involvement.
- Iodinated contrast — metformin: because metformin accumulates and risks lactic acidosis if CA-AKI develops, ESUR guidance is to withhold metformin from the time of contrast administration and for 48 hours afterward in patients with eGFR <60 (or when a large contrast volume is given), resuming only after renal function is confirmed stable. Metformin is not stopped routinely in patients with normal renal function receiving small volumes.
- Iodinated contrast — thyroid: large iodine loads can precipitate hyperthyroidism in susceptible patients (Jod–Basedow effect); note active thyrotoxicosis.
- Gadolinium (GBCA) — renal function: in severe renal failure (eGFR <30) gadolinium can cause nephrogenic systemic fibrosis (NSF); macrocyclic agents carry lower risk than linear agents, and GBCAs are avoided or used with great caution at eGFR <30 and in dialysis-dependent patients.
Provided image
SELF-CHECK
A 60-year-old man on metformin with an eGFR of 40 mL/min/1.73 m² is booked for a contrast-enhanced CT. Regarding the metformin, what does pre-imaging screening require?
A. No action; metformin is unrelated to iodinated contrast
B. Withhold metformin from the time of contrast and for 48 hours, resuming only after renal function is confirmed stable
C. Permanently stop metformin before any future imaging
D. Switch the patient to gadolinium contrast instead of iodinated contrast
Reveal Answer
Answer: B. Withhold metformin from the time of contrast and for 48 hours, resuming only after renal function is confirmed stable
ESUR guidance advises withholding metformin from the time of iodinated contrast administration and for 48 hours afterward in patients with eGFR <60 (or with large contrast volumes), then resuming after stable renal function is confirmed, to avoid lactic acidosis should contrast-associated AKI occur. Permanent discontinuation is unwarranted. Gadolinium is an MRI agent and does not enhance CT, so it is not a substitute for iodinated contrast in a CT study.
Screening for Magnetic-Field Exposure — The MRI Safety Checklist
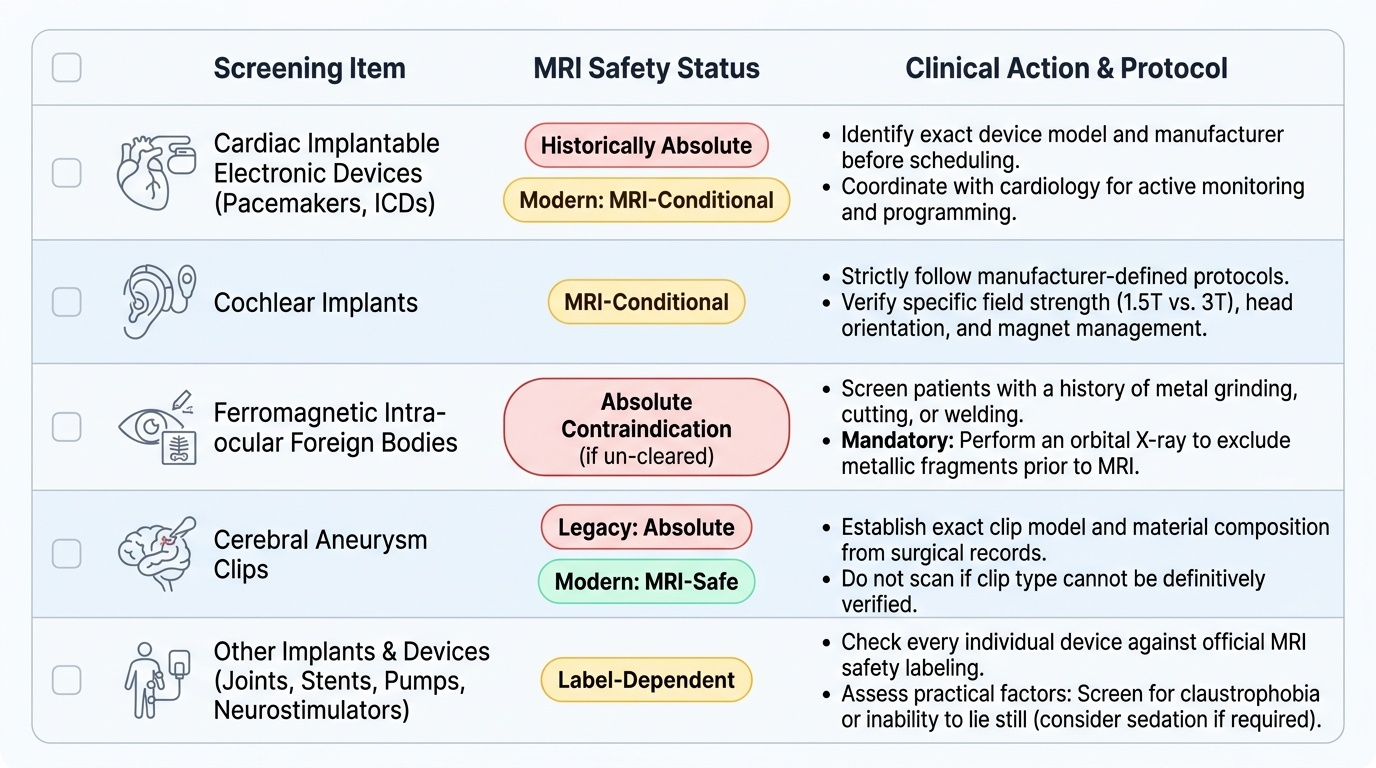
Screening for magnetic-field exposure is the safety step unique to MRI, and it exists because the MRI environment is hazardous in a way that has nothing to do with radiation: a powerful static magnetic field (typically 1.5–3 Tesla) exerts strong force on ferromagnetic objects, and the radiofrequency pulses can heat tissue and induce currents in conductive implants. The categorical teaching point is that MRI is NOT contraindication-free — stating that 'MRI has no contraindications' is both an examination error and a genuine patient-safety hazard. Every patient must be screened against a defined checklist before entering the magnet, and a positive answer does not always mean 'no MRI'; many modern implants are MRI-conditional, meaning they are safe only under the manufacturer's defined conditions (specific field strength, positioning, and monitoring). The screening task is to identify the device precisely and check its status, never to assume.
- Cardiac implantable electronic devices (pacemakers and ICDs): traditionally an absolute contraindication; many newer devices are MRI-conditional and may be scanned under a specific protocol with cardiology involvement. Identify the exact device before booking.
- Cochlear implants: a recognised contraindication unless the specific device is certified MRI-conditional and the manufacturer's protocol (field strength, head orientation, magnet management) is followed.
- Ferromagnetic intra-ocular foreign bodies: a hazard in patients with a history of metal grinding, cutting or welding; a tiny intra-ocular metal fragment can move in the field and injure the eye. An orbital X-ray to exclude metallic fragments is mandatory before MRI in any such patient.
- Cerebral aneurysm clips: older ferromagnetic clips may move in the field — establish the clip type before MRI; many modern clips are non-ferromagnetic and MRI-safe.
- Other implants and devices: joint prostheses, stents, drug-infusion pumps, neurostimulators and retained pacing wires must each be checked against their MRI labelling; claustrophobia and inability to lie still are practical screening considerations that may require sedation or an alternative modality.
Provided image
Putting It Together — Suitability Decisions Across Common Clinical Requests
The clinical value of screening is realised when the three checks are run together against a real request and converted into one of three decisions: proceed as requested, modify the request (a different protocol, withholding a drug, premedicating, or hydrating), or choose an alternative modality altogether. Applied screening is what separates a clinician who reflexively orders the most powerful study from one who orders the safest study that answers the question — and it is exactly the judgement that competency RD2.1 is written to develop. The integration is straightforward once the habit is built: identify which hazards the requested study carries, ask the relevant screening questions for each of those hazards, and let any positive answer drive the decision toward proceed, modify, or substitute. The following worked examples show the integrated screen in action across the three hazard domains.
- Contrast-enhanced CT in a patient with CKD: the radiation screen confirms justification; the iodinated-contrast screen finds eGFR 28 and metformin use → modify: discuss with radiology, consider a non-contrast protocol or alternative, withhold metformin per protocol, and hydrate if contrast proceeds.
- MRI brain in a metal-worker with headaches: the magnetic-field screen flags possible intra-ocular metal → modify the pathway: orbital X-ray first; if a fragment is present, MRI is contraindicated and CT is the alternative.
- Abdominal imaging in early pregnancy: the radiation screen flags the fetus → choose an alternative: ultrasound first, MRI (without gadolinium where avoidable) if further characterisation is needed.
- Contrast study in a patient with prior severe contrast reaction: the contrast screen flags anaphylactoid history → modify: premedicate and involve radiology, or select a study that does not require that agent.
Documentation closes the loop: the screening findings (allergy/reaction history, eGFR with date, pregnancy status, implant status) and the resulting decision should be recorded on the request and in the notes, and informed consent for contrast obtained where required. A screen that is performed but not documented leaves the downstream team unable to act on it and the clinician unable to demonstrate that suitability was assessed.
SELF-CHECK
A 45-year-old man with progressive leg weakness needs an MRI lumbar spine. On screening he reports a cochlear implant placed two years ago. What is the correct screening-driven action?
A. Proceed with MRI, since cochlear implants are generally MRI-safe
B. Identify the specific implant and check the manufacturer's documentation to determine whether it is MRI-conditional before proceeding
C. Scan at 3 Tesla rather than 1.5 Tesla to reduce the magnetic hazard
D. Cancel all spinal imaging permanently
Reveal Answer
Answer: B. Identify the specific implant and check the manufacturer's documentation to determine whether it is MRI-conditional before proceeding
A cochlear implant is a recognised MRI contraindication UNLESS the specific device is certified MRI-conditional and its manufacturer protocol (field strength, head orientation, magnet management) is followed. The correct screening action is to identify the exact device and verify its MRI status, never to assume safety. Higher field strength increases, not decreases, the magnetic hazard. If the implant is a true contraindication, an alternative such as CT myelography may be considered, but the first step is device identification.
CLINICAL PEARL
Pearl 1 — Iodine 'allergy' and shellfish allergy do NOT predict contrast reactions. A common but incorrect reason to cancel a needed contrast study. The relevant screening item is a prior reaction to iodinated contrast itself (and severe atopy/asthma), not a reported iodine or shellfish allergy. Screen for the right thing.
Pearl 2 — eGFR <30 is the number to remember for BOTH contrast families. It is the high-risk threshold for iodinated contrast (CA-AKI) and for gadolinium (NSF). Withhold metformin at the time of iodinated contrast and for 48 h when eGFR <60 or a large volume is used.
Pearl 3 — 'MRI-conditional' is not 'MRI-safe.' A conditional device is safe ONLY under the manufacturer's defined conditions. The screening task for any implant is to identify the exact device and check its labelling — never to wave a patient through on the assumption that 'modern implants are fine.'
Pearl 4 — AERB, not NRC/ICRP, is India's regulator. Justification of every ionising study is mandated by the AERB under the Atomic Energy Act 1962; cite AERB as the Indian authority.
Self-Assessment — Screening Scenarios
Use these scenario questions to test your grasp of pre-imaging suitability screening across the three hazard domains. Write your answer before reading the discussion, and in each case name the screening domain involved and the decision it drives.
Scenario A: A 70-year-old diabetic man with an eGFR of 26 mL/min/1.73 m², taking metformin, is referred for a contrast-enhanced CT to stage a suspected renal tumour. He reports no prior contrast reaction. What does screening require?
Discussion: This is a contrast (and radiation) screen. The eGFR of 26 is below the high-risk threshold of 30, so CA-AKI risk is significant: discuss with radiology whether a non-contrast or alternative protocol (e.g. MRI without gadolinium, or with a macrocyclic agent only if essential) can stage the tumour; if iodinated contrast is judged necessary, use the lowest volume with hydration. Withhold metformin from the time of contrast and for 48 hours, resuming after stable renal function is confirmed. Document eGFR, the decision, and the metformin plan.
Scenario B: A 32-year-old woman at 8 weeks of pregnancy has suspected renal colic with haematuria. The surgical team wants a CT KUB. What is the most defensible screening-driven plan?
Discussion: This is a radiation screen with a positive pregnancy result. Begin with ultrasound (no ionising radiation) to look for hydronephrosis/calculi; if inconclusive and further characterisation is essential, MRI (without gadolinium where avoidable) is the next non-ionising step. CT KUB exposes the fetus to ionising radiation and is reserved for situations where the alternatives have failed and a definitive answer is essential, with the lowest feasible dose. Establish and document the pregnancy status and the rationale.
Scenario C: A 55-year-old man with a permanent pacemaker needs an MRI of the brain for suspected acoustic neuroma. How should screening proceed?
Discussion: This is a magnetic-field screen with a positive cardiac-device finding. Do not assume the pacemaker is a contraindication and do not assume it is safe: identify the exact device and lead system and determine whether it is MRI-conditional. If conditional, MRI may proceed under the manufacturer's protocol with cardiology involvement and device interrogation before and after the scan. If it is a non-conditional (legacy) device, MRI is contraindicated and a contrast-enhanced CT or alternative pathway is used. Document the device identification and the decision.