Page 10 of 17
RD5.4 | Device Position on Adult and Pediatric ICU Chest X-ray — SDL Guide
Learning Objectives
- Apply a systematic 'tubes-and-lines-first' read to an ICU/portable chest radiograph.
- State and recognise the correct radiographic position of an endotracheal tube, central venous catheter and nasogastric tube.
- Recognise the common malpositions of each device and the clinical harm each causes.
- Perform the mandatory post-insertion complication check, especially for pneumothorax after central-line or other insertion.
- Describe how paediatric device-position targets differ from adult targets and why the short paediatric airway makes tube migration more dangerous.
INSTRUCTIONS
Intensive-care patients are kept alive by tubes and lines, and a device in the wrong place can be as dangerous as no device at all — an endotracheal tube in the right main bronchus collapses the opposite lung, a feeding tube in the airway delivers feed into the lungs, and a central line can cause a pneumothorax on insertion. The portable chest X-ray is the standard tool for confirming device position after insertion and on the daily ICU round, and the competency RD5.4 asks you to interpret the normal and abnormal position of these devices on adult AND paediatric ICU films. This module builds the disciplined 'tubes-and-lines-first' read: trace each device to its tip, judge it against its target landmark, recognise the dangerous malpositions, and — every time — search for the complication. Paediatric differences, where the short airway magnifies the danger of small errors, run throughout.
References
- Sutton's Textbook of Radiology and Imaging, 7th edition, The Chest in Intensive Care — tubes, lines and catheters (textbook)
- Grainger & Allison's Diagnostic Radiology, 7th edition, Imaging in the Intensive Care Unit (textbook)
- Atomic Energy Regulatory Board (AERB) Safety Code for Diagnostic Radiology — portable radiography and paediatric dose optimisation (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A patient in the ICU is intubated for respiratory failure, and the post-intubation portable chest X-ray is brought to the resident. She confirms the endotracheal tube is in the trachea and signs off — but she does not check the DEPTH. Over the next hour the patient's left chest stops moving and the oxygen saturation falls. A repeat film shows the tube tip sitting in the RIGHT main bronchus, ventilating only the right lung, while the left lung has collapsed. The fix is simple — withdraw the tube a few centimetres so its tip lies above the carina — but only if someone reads the position correctly. The same lesson repeats with every device in the unit: a central line whose tip is in the right atrium can trigger arrhythmias, a nasogastric tube that coiled into the airway can deliver feed into the lungs, and a freshly inserted central line can cause a pneumothorax. On the ICU film, confirming that every tube and line is in the right place — and that its insertion caused no complication — is a daily, life-saving interpretation skill.
WHY THIS MATTERS
Junior doctors are routinely the first to see the post-insertion and morning ICU chest films, and acting on a malpositioned device is squarely their responsibility. The NMC competency RD5.4 asks specifically for interpretation of the normal and abnormal position of devices on the chest X-ray of ADULT and PAEDIATRIC ICU patients, recognising that critical-care imaging is a core generalist skill and that children are not small adults. The harms of missing a malposition are immediate and serious: an endotracheal tube too low causes single-lung ventilation and contralateral collapse (or, too high, accidental extubation); a central venous catheter tip in the right atrium can provoke arrhythmias or, over time, perforation; a misplaced nasogastric tube in the airway leads to aspiration pneumonia if feed is started; and any central-line insertion can be complicated by a pneumothorax that must be found before the line is used. Because the portable film is an AP supine projection, it carries its own caveats (heart size cannot be judged), and because the paediatric airway and great vessels are short, small migrations are proportionally large and more dangerous. This makes the systematic device check a daily, examinable patient-safety task, not a radiologist's preserve.
RECALL
Before reading further, recall the anatomy and the normal-film foundations this device check depends on:
- The normal CXR landmarks (RD5.1): the trachea (midline, air-filled), the carina (the tracheal bifurcation, typically projecting around the T4–T5 level), the superior vena cava (SVC) and its junction with the right atrium (the cavoatrial junction), and both hemidiaphragms.
- Mediastinal venous anatomy: the SVC drains into the right atrium; a central line advanced from the neck or arm should sit with its tip in the lower SVC at the cavoatrial junction, not within the heart.
- Airway vs oesophagus: the trachea lies anterior; the oesophagus runs behind it and descends to the stomach below the left hemidiaphragm — a feeding tube must follow the oesophagus, not the airway.
- Projection caveat (RD5.1): the ICU film is an AP/supine PORTABLE film, so the heart and mediastinum are magnified and true heart size cannot be judged.
- Pneumothorax recognition (RD5.3): a lung edge with absent peripheral markings — the complication to exclude after any line insertion.
If the carina or cavoatrial-junction landmarks are unclear, a quick review of the normal CXR now will make the device targets below far easier to apply.
Why Checking Every Tube and Line on the ICU Film Is a Daily Safety Task
The ICU chest radiograph is requested for two recurring reasons, and both make device-position checking a daily, decision-driving task rather than an academic exercise. The first is the POST-INSERTION confirmation film: after intubation, central-line placement, nasogastric-tube insertion or chest-drain placement, a chest X-ray confirms that the device is correctly positioned AND that the insertion caused no complication before the device is used. The second is the ROUTINE daily film, on which devices can migrate over time — an endotracheal tube creeps with neck movement, a nasogastric tube is partly pulled back, a central line tip shifts — so each must be re-confirmed. In both settings the reader's job is the same: confirm position against the correct landmark, recognise any dangerous malposition, and search for the complication. The competency frames this for both adult and paediatric patients, and the consequences are immediate.
The harms of an unrecognised malposition are concrete and each triggers a specific action:
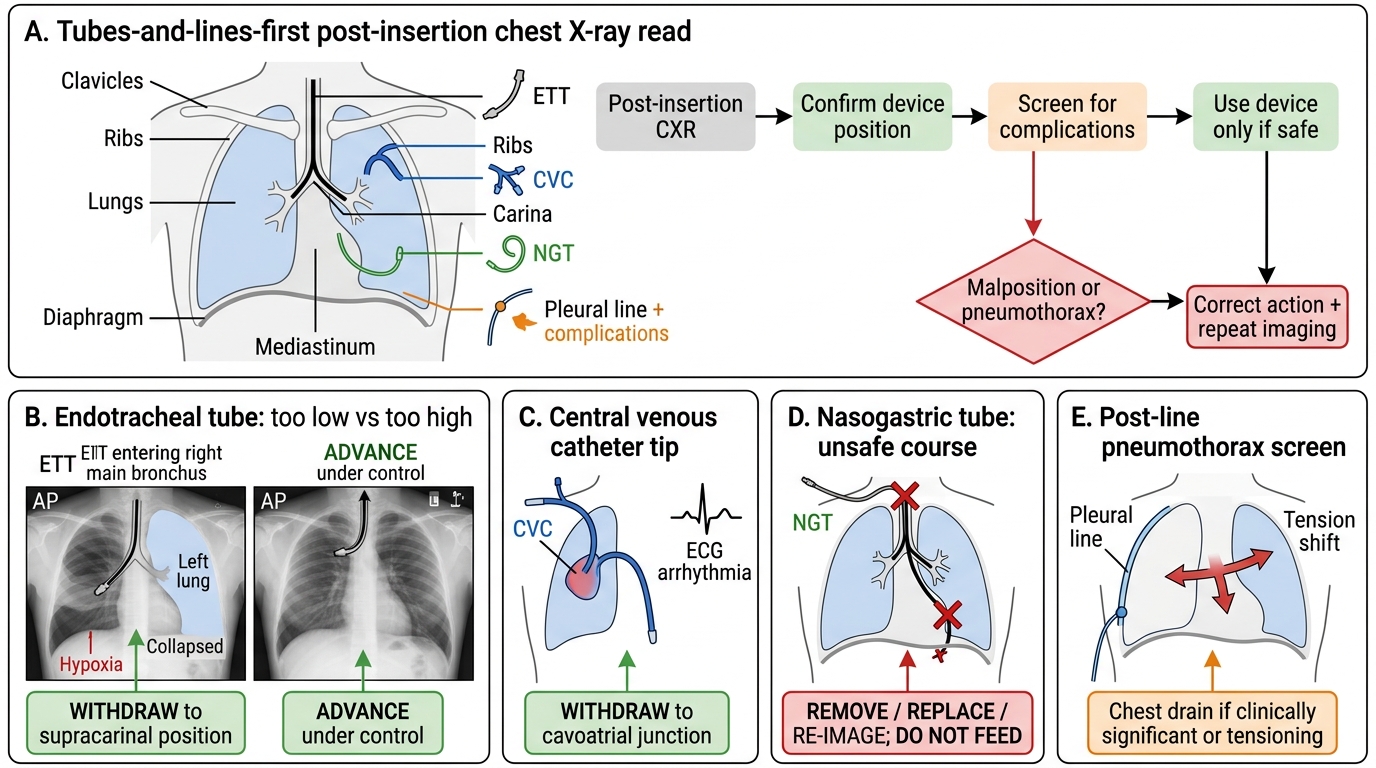
Post-Insertion Chest X-Ray: Tubes, Lines and Corrective Actions
- Endotracheal tube too LOW (in the right main bronchus) → single-lung ventilation, LEFT lung collapse, hypoxia → WITHDRAW the tube to a supracarinal position.
- Endotracheal tube too HIGH → risk of accidental extubation → ADVANCE under control.
- Central venous catheter tip in the right atrium → arrhythmias, risk of perforation → WITHDRAW to the cavoatrial junction.
- Nasogastric tube in the airway or above the diaphragm → aspiration if fed → REMOVE/REPLACE and re-image; do NOT feed until confirmed.
- Pneumothorax after line insertion → may tension → chest drain → exclude on EVERY post-line film.
The unifying discipline is a 'tubes-and-lines-first' read in which detection of a malposition is always coupled to its corrective action.
Governing Principles — Portable AP Films, Anatomical Landmarks and a Tubes-and-Lines-First Read
Three governing principles make the ICU device read reliable. The first is that the ICU film is almost always an AP SUPINE PORTABLE film, which changes how you read it: the heart and mediastinum are magnified (you CANNOT judge true heart size or call cardiomegaly), the scapulae often overlie the lungs, and lordotic angulation is common. You read this film for tubes, lines and acute lung change — not for cardiac size. The second principle is to anchor every device to its correct ANATOMICAL LANDMARK, because 'looks about right' is not a standard. The key landmarks are the carina (for the endotracheal tube tip), the lower SVC at the cavoatrial junction (for the central venous catheter tip), and the left hemidiaphragm/stomach (for the nasogastric tube tip). The carina is the single most important reference for tube depth and typically projects around the T4–T5 vertebral level on a frontal film.
The third principle is the EFFECT OF NECK POSITION on the endotracheal tube, a frequent source of apparent malposition: the tube tip moves toward the carina with neck FLEXION ('the tube goes where the chin goes') and away from it with neck EXTENSION, so the tip position must be judged with the neck in a neutral position and the neck position noted.
⚑ AI image — pending faculty review (auto-QA score 8/10; best of 3 attempts)
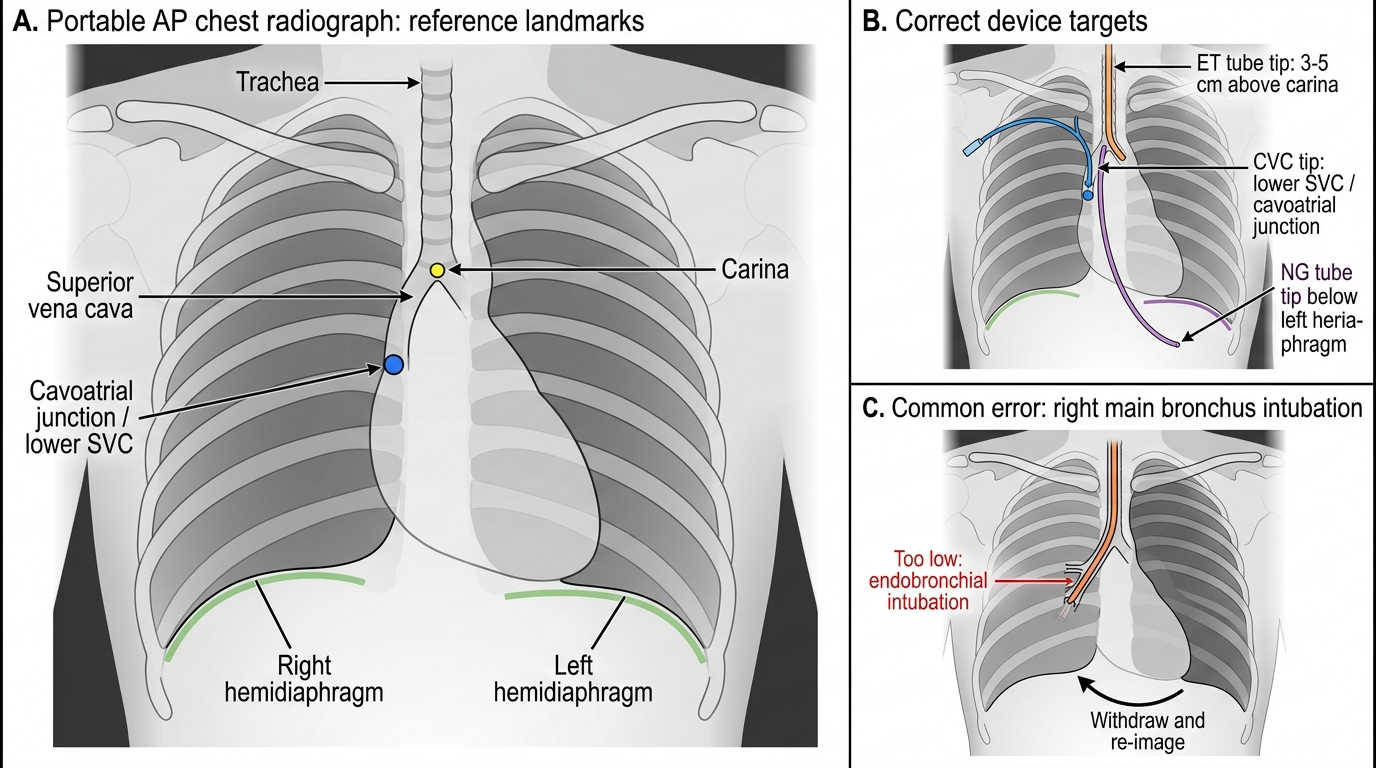
Portable AP Chest Radiograph Landmarks for Tube and Line Positioning
- Carina — reference for the ET tube tip (target ~3–5 cm above it, neutral neck).
- Cavoatrial junction / lower SVC — target for the CVC tip.
- Left hemidiaphragm / stomach — the NG tube tip must lie clearly below it, in the midline-following oesophageal course.
With these landmarks fixed, the read becomes a disciplined 'tubes-and-lines-first' sweep — trace each device, judge it against its landmark, then search for complications — performed before the routine lung review.
SELF-CHECK
A post-intubation portable chest film shows the endotracheal tube tip in the right main bronchus. Clinically the left chest is not moving well. What is the correct immediate interpretation and action?
A. The tube is correctly placed; no action needed
B. The tube is too low (endobronchial), causing left-lung hypoventilation/collapse; withdraw it so the tip lies ~3–5 cm above the carina, then re-image
C. Advance the tube further to secure the airway
D. The film cannot assess tube position; rely on auscultation alone
Reveal Answer
Answer: B. The tube is too low (endobronchial), causing left-lung hypoventilation/collapse; withdraw it so the tip lies ~3–5 cm above the carina, then re-image
An endotracheal tube tip in the right main bronchus is too LOW (endobronchial intubation); it ventilates only the right lung and causes left-lung hypoventilation or collapse. The correct action is to WITHDRAW the tube so its tip lies approximately 3–5 cm above the carina (neutral neck), then re-image to confirm. Advancing it would worsen the problem. The chest film is precisely the tool used to confirm tube depth against the carina; auscultation alone is unreliable.
Method — Locating the ET Tube, CVC, NG Tube and Other Devices Step by Step
The method is to trace EACH device from its point of entry to its tip, judge the tip against its landmark, and only then move to the next device — never assuming a device is correct because it is present. Work through the devices in a fixed order so none is forgotten, and finish, every single time, with a deliberate search for an insertion complication. Below, each device is given its correct target and the way to trace it.
Endotracheal (ET) tube: trace it down the air-filled trachea in the midline. The correct tip lies approximately 3–5 cm above the carina with the neck in a neutral position. Too low risks right-main-bronchus intubation (left-lung collapse); too high risks accidental extubation. Note the neck position, because flexion drives the tip down and extension pulls it up.
Central venous catheter (CVC): trace it from the neck (internal jugular) or chest (subclavian) along the expected venous course. The correct tip lies at the cavoatrial junction / lower SVC — not curling into the right atrium (arrhythmia/perforation risk) and not heading up the opposite brachiocephalic vein or into the azygos.
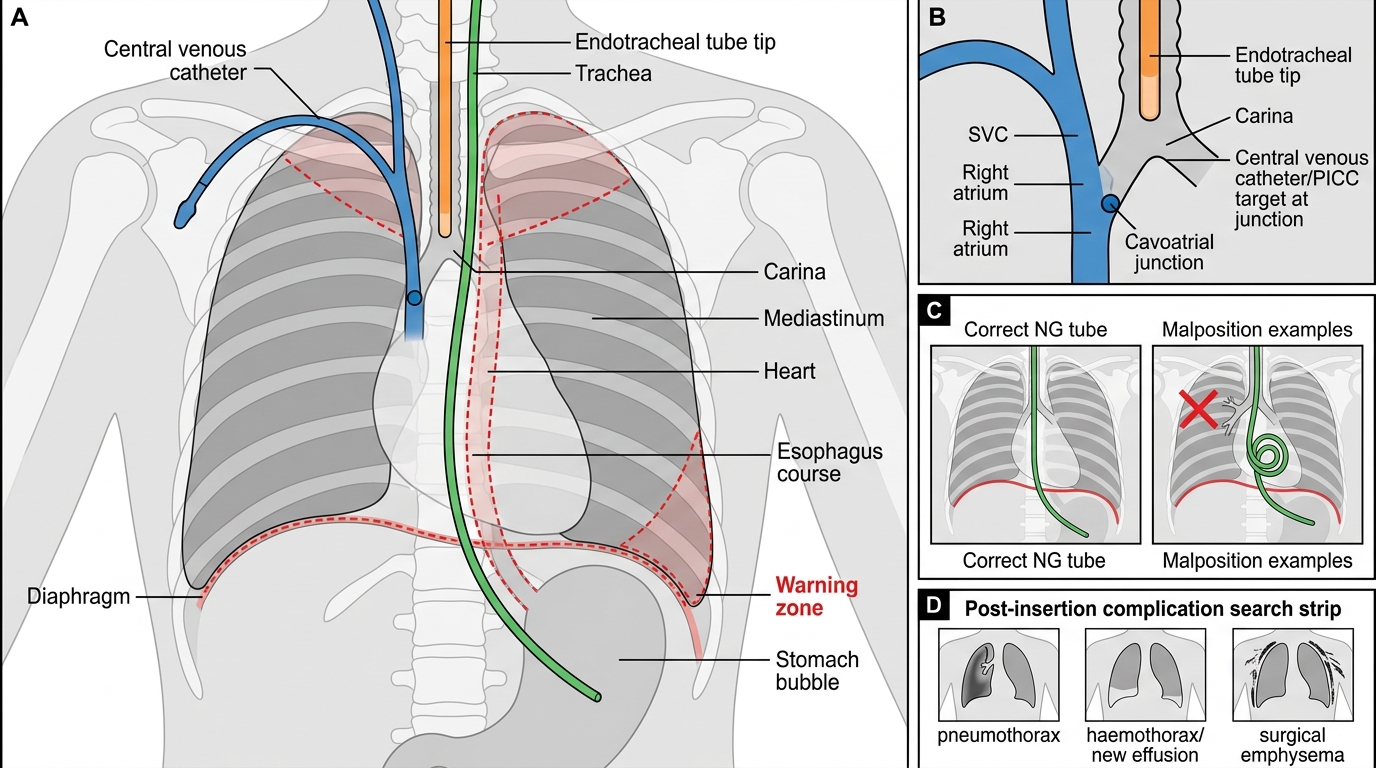
Correct Positioning of ICU Tubes on Chest Radiograph
Nasogastric (NG) tube: the critical SAFETY check. The tube must descend in the MIDLINE following the oesophagus, bisect the carina, remain to the left of the spine inferiorly, and have its tip clearly below the left hemidiaphragm in the stomach. A tube that deviates into a bronchus, coils in the pharynx/oesophagus, or whose tip is above the diaphragm is MALPOSITIONED — do NOT feed until a correct position is confirmed (radiography is the gold-standard confirmation).
Other devices, briefly: a PICC line (from the arm) targets the same cavoatrial junction; temporary pacing wires/leads should project over the expected cardiac chamber; a chest drain should run toward the apex (for air) or base (for fluid) with its last side-hole inside the pleural cavity; a Swan-Ganz (pulmonary artery) catheter tip should sit in a main/proximal pulmonary artery, not wedged peripherally.
Always finish with the complication search: after any insertion, deliberately look for a pneumothorax, a haemothorax/new effusion, or surgical emphysema before the device is used.