Page 11 of 17
RD5.4 | Device Position on Adult and Pediatric ICU Chest X-ray — SDL Guide (Part 2)
Interpretation of Findings — Correct vs Malpositioned Devices and the Mandatory Complication Check
Interpretation means deciding, for each device, whether it is correctly positioned or malpositioned, naming the specific malposition and its harm, and then performing the mandatory complication check — and doing all of this with the adult-versus-paediatric difference in mind. A correct device sits exactly at its anatomical landmark; a malpositioned one departs from it in a characteristic, recognisable way, and each departure carries a defined consequence and a defined corrective action, so interpretation is never simply 'present or absent' but always 'correctly placed, or malpositioned and how.' The skill is to convert what you see into a decision: confirm the device against its target landmark, and if it is wrong, state precisely what is wrong, what harm it threatens, and what should be done about it. Only once every device has been judged this way do you turn to the complication search that every post-insertion film demands. The table below consolidates the target, the common malposition and the clinical consequence for the three core devices.
Provided image
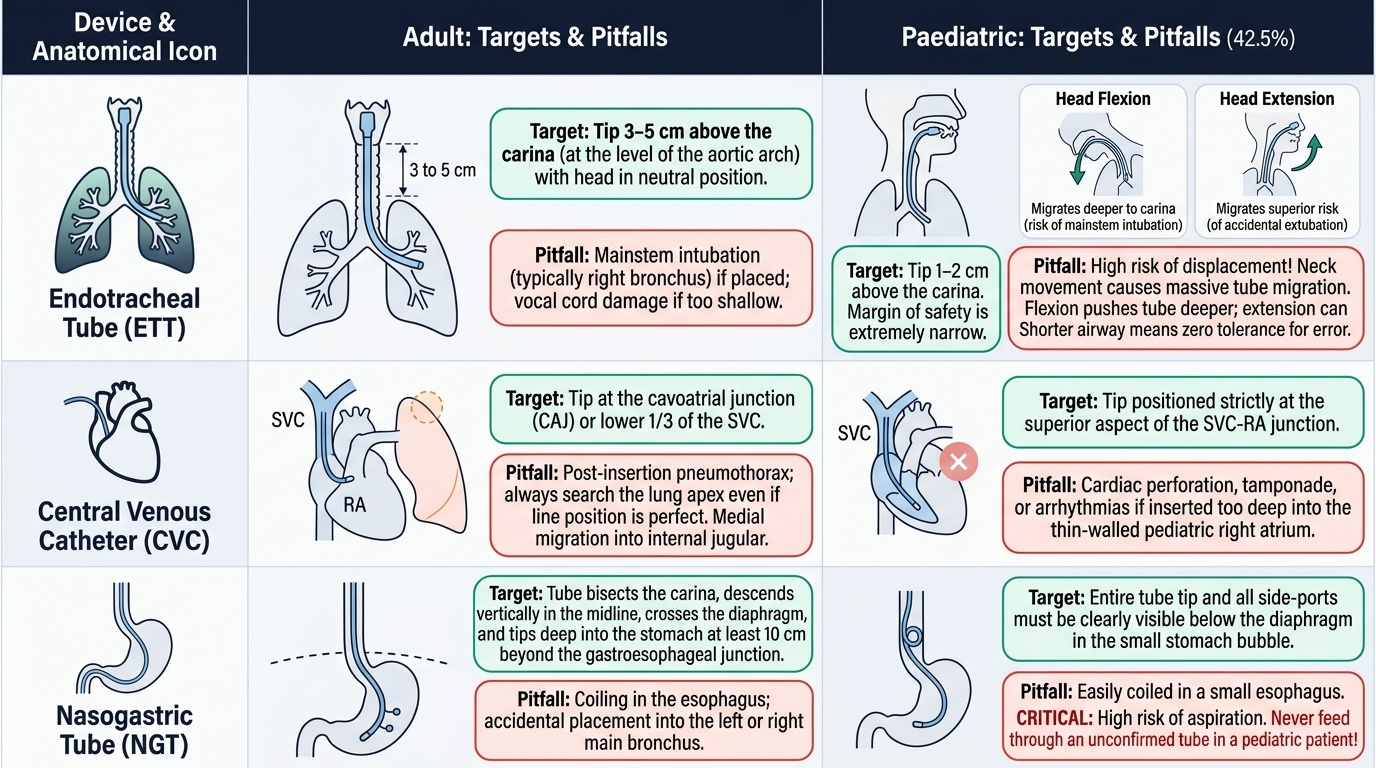
| Device | Correct (target) position | Common malposition | Consequence |
|---|---|---|---|
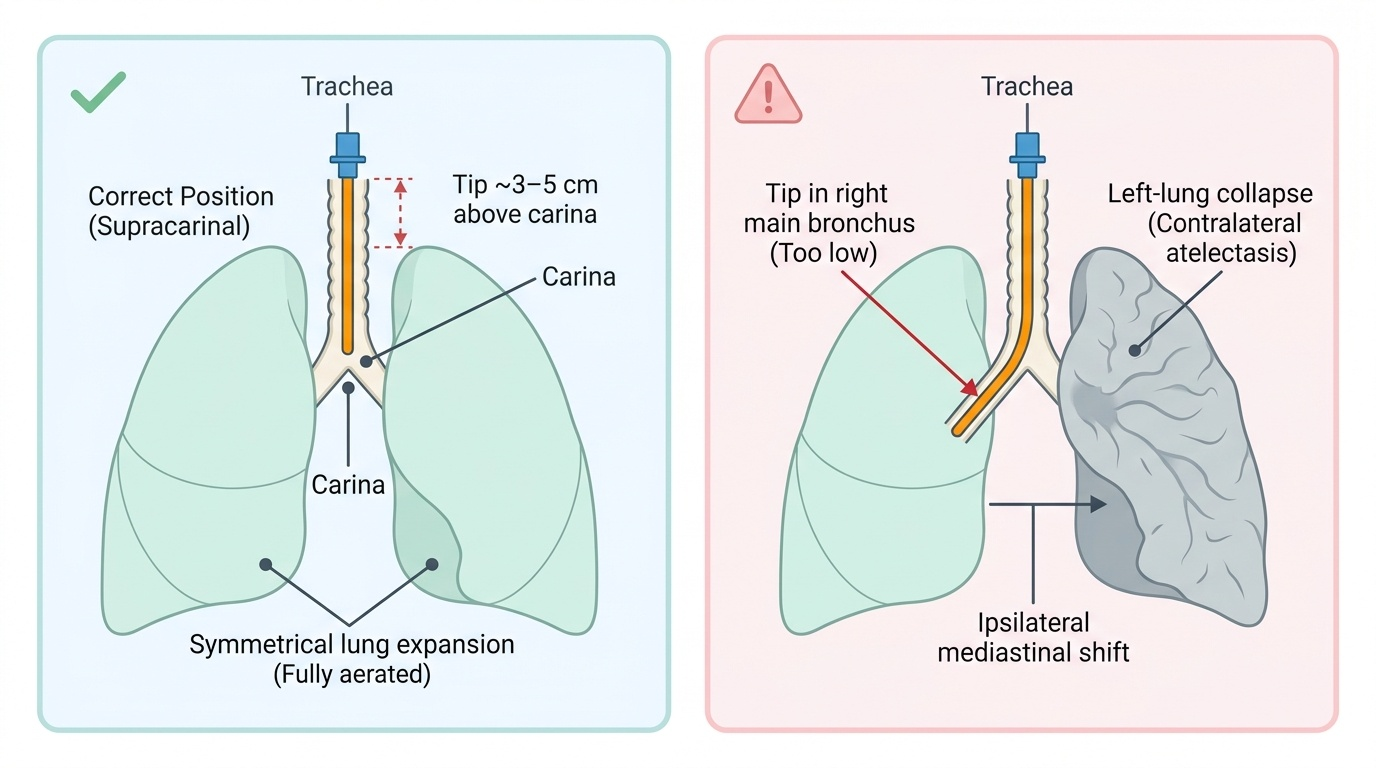
| ET tube | Tip ~3–5 cm above the carina (neutral neck) | Tip in right main bronchus (too low) / too high | Left-lung collapse / accidental extubation |
| CVC | Tip at cavoatrial junction / lower SVC | Tip in right atrium, or aberrant vein | Arrhythmia/perforation; ineffective/aberrant delivery |
| NG tube | Tip below left hemidiaphragm, midline course | Coiled in airway/oesophagus, tip above diaphragm | Aspiration if fed; ineffective feeding |
The classic, named malposition to recognise instantly is the endobronchial endotracheal tube with contralateral collapse:
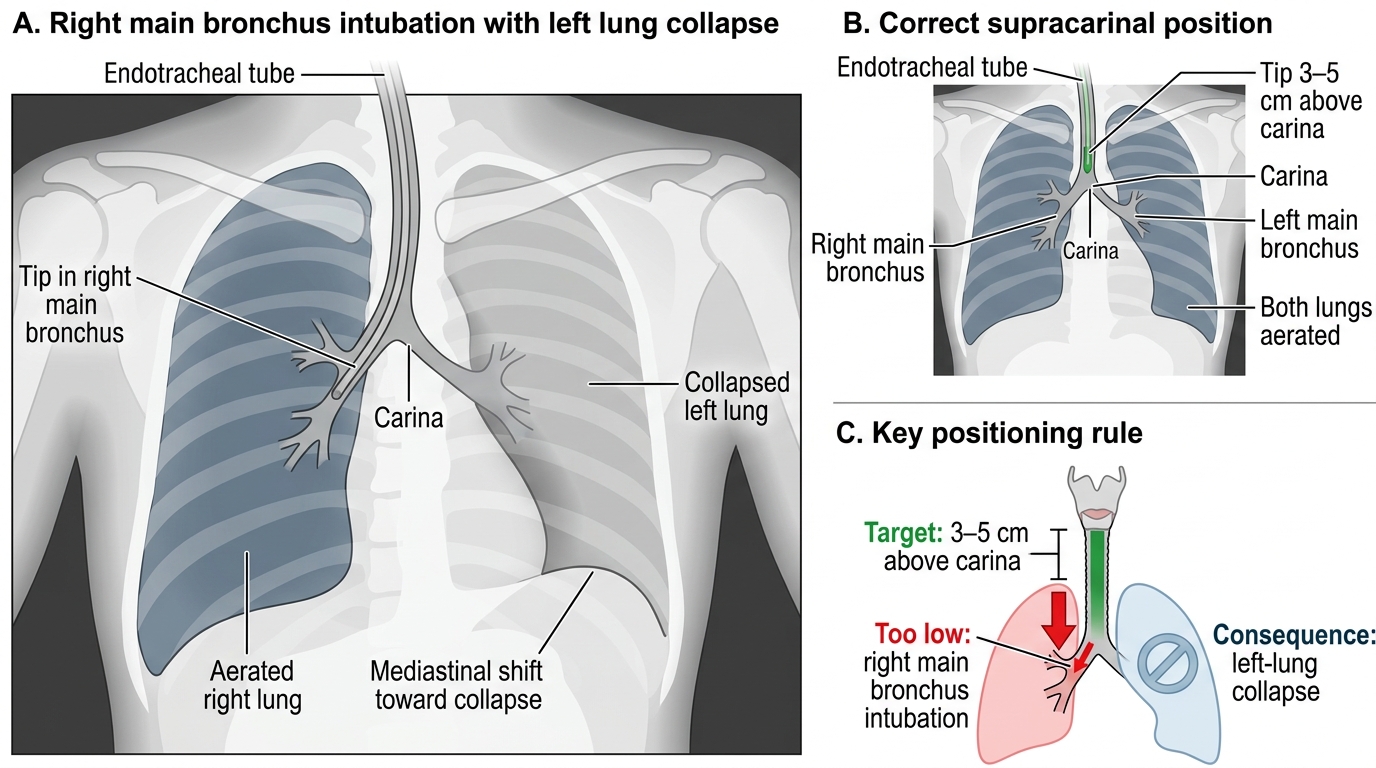
Endotracheal Tube Position: Correct Supracarinal Placement vs Right Main Bronchus Malposition
The MANDATORY complication check after any insertion is for a pneumothorax (a lung edge with absent peripheral markings — recall RD5.3; on a supine film look also for the deep sulcus sign), and for a haemothorax or surgical emphysema. This check is non-negotiable on every post-line film, because a line may be perfectly positioned yet its insertion may have caused a pneumothorax that will tension if missed.
The PAEDIATRIC differences are critical and competency-specified: the child's airway and great vessels are SHORT, so the absolute safe-position margins are smaller and a few millimetres of migration is proportionally large; the ET tube moves more with neck flexion/extension; and target depths are age/size-specific rather than the adult 3–5 cm figure. The same systematic check applies, but with paediatric reference values and a lower threshold for re-imaging after any repositioning.
Applied Practice — Reviewing a Post-Insertion and a Routine ICU Film
Applied practice means performing the full tubes-and-lines-first review on real ICU films and coupling each finding to its action, because in critical care a recognised malposition demands an immediate correction rather than a note for later. Rehearse the five-step sequence below until it is a reflex: first, identify every device on the film, so none is overlooked; second, trace each device from its point of entry to its tip; third, judge each tip against its landmark target (carina for the ET tube, cavoatrial junction for the CVC, left hemidiaphragm/stomach for the NG tube); fourth, deliberately search for an insertion complication such as a pneumothorax; and fifth, act on every abnormality with its specific correction and re-imaging. The worked cases that follow apply this single discipline to a post-insertion film, a routine daily film, an NG-tube safety check and a paediatric film, showing that the same sequence scales across every situation the ICU presents.
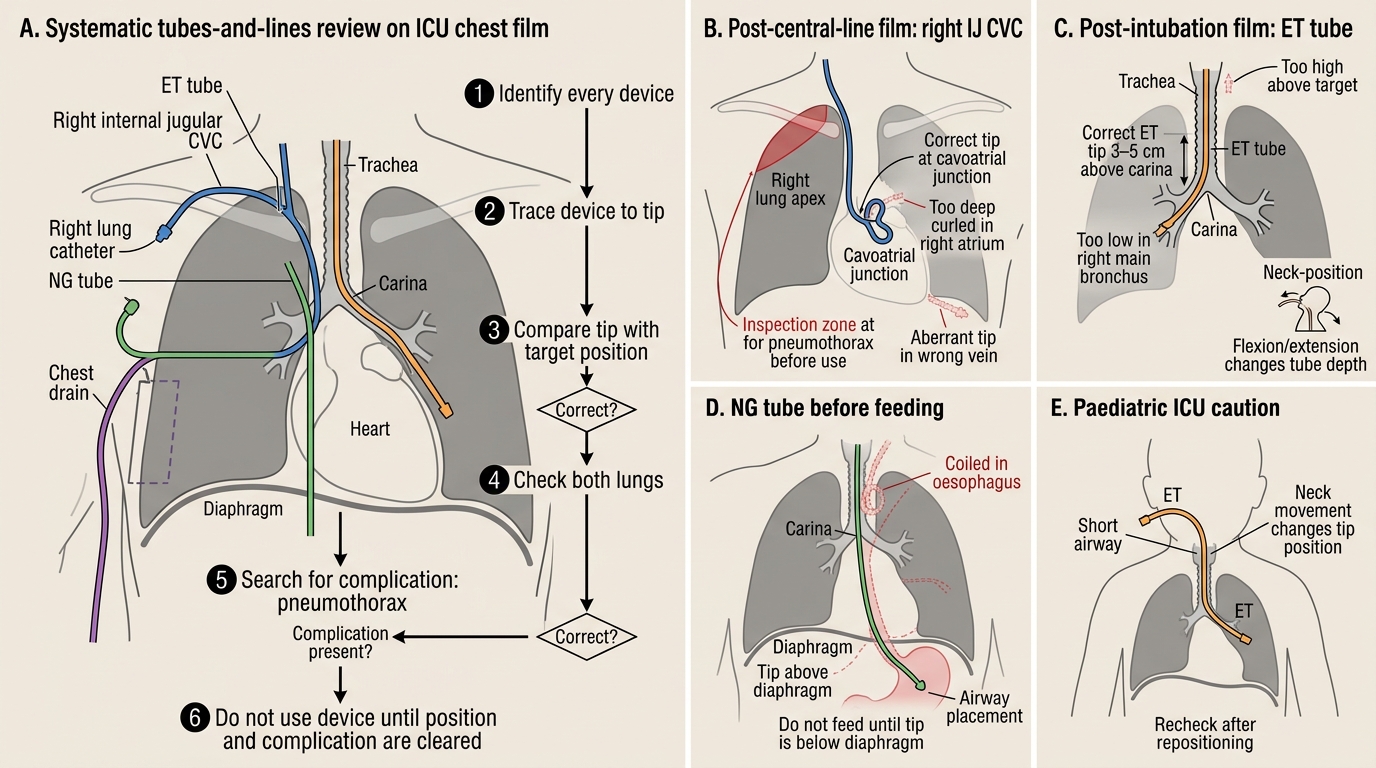
Systematic ICU Chest Film Tubes-and-Lines Review
Worked case 1 — post-central-line film: a right internal-jugular CVC has just been placed. CHECK: trace the line to its tip — is it at the cavoatrial junction (correct) or curled in the right atrium (withdraw) or in an aberrant vein (reposition)? Then, mandatorily, search for a PNEUMOTHORAX before the line is used; if present and significant, insert a chest drain. Do not use the line until both position and complication are cleared.
Worked case 2 — post-intubation film (the hook): an ET tube is in place. CHECK: trace it down the trachea — is the tip ~3–5 cm above the carina (correct), or in the right main bronchus (too low → withdraw → re-image), or too high (advance)? Note the neck position before judging. Confirm both lungs are aerated.
Worked case 3 — routine daily film with an NG tube: before feeding is restarted, CHECK the NG tube — does it descend in the midline, bisect the carina, and have its tip clearly below the left hemidiaphragm in the stomach? If it is coiled in the oesophagus/airway or its tip is above the diaphragm, do NOT feed; replace and re-image.
Worked case 4 — paediatric ICU film: the same review, but with PAEDIATRIC targets — remember the short airway means small ET-tube migrations are proportionally large and the tube moves more with neck position, so use age/size-specific reference depths and re-image after any repositioning. The cross-cutting applied lesson is that every device review ends with the complication search and that every malposition is paired with its specific corrective action (withdraw, advance, reposition or replace) and re-imaging.
SELF-CHECK
Before restarting feeds, you review the nasogastric tube on an ICU chest film. Which finding confirms the tube is SAFELY positioned in the stomach?
A. The tube tip lies in the right main bronchus
B. The tube descends in the midline, bisects the carina, and its tip lies clearly below the left hemidiaphragm in the stomach
C. The tube is coiled in the lower oesophagus above the diaphragm
D. The tube tip is at the cavoatrial junction
Reveal Answer
Answer: B. The tube descends in the midline, bisects the carina, and its tip lies clearly below the left hemidiaphragm in the stomach
A safely positioned nasogastric tube follows the oesophagus in the MIDLINE, bisects the carina, stays to the left of the spine inferiorly, and has its tip clearly BELOW the left hemidiaphragm in the stomach — radiography is the gold-standard confirmation before feeding. A tube in a bronchus or coiled above the diaphragm is malpositioned and must not be used for feeding (aspiration risk). The cavoatrial junction is the target for a central venous catheter, not a nasogastric tube.
SELF-CHECK
Which statement about device-position assessment on the chest X-ray of a PAEDIATRIC ICU patient is correct?
A. Paediatric targets are identical to adult targets, including the 3–5 cm supracarinal ET tube figure
B. Because the paediatric airway and great vessels are short, small device migrations are proportionally large and more dangerous, so age/size-specific reference positions are used and there is a low threshold to re-image after repositioning
C. The complication check for pneumothorax does not apply to children
D. Heart size can be reliably assessed on a paediatric portable AP film
Reveal Answer
Answer: B. Because the paediatric airway and great vessels are short, small device migrations are proportionally large and more dangerous, so age/size-specific reference positions are used and there is a low threshold to re-image after repositioning
Children are not small adults: the short paediatric airway and great vessels mean a few millimetres of tube or line migration is proportionally large and more dangerous, the ET tube moves more with neck flexion/extension, and target depths are age/size-specific rather than the adult 3–5 cm figure — with a low threshold to re-image after any repositioning. The post-insertion pneumothorax check still applies, and heart size cannot be reliably judged on any portable AP film, adult or paediatric.
CLINICAL PEARL
Pearl 1 — Judge the ET tube against the CARINA, with the neck noted. Target tip ~3–5 cm above the carina in a neutral neck. The tube tip moves DOWN with neck flexion and UP with extension — 'the tube goes where the chin goes' — so always note neck position before calling a tube too low or too high.
Pearl 2 — Never feed through an unconfirmed NG tube. A safe NG tube runs in the midline, bisects the carina and has its tip clearly below the left hemidiaphragm; radiography is the gold-standard check. A tube in the airway or above the diaphragm is a potential aspiration disaster — replace and re-image before feeding.
Pearl 3 — Every post-line film gets a pneumothorax check. A central line can be perfectly positioned and still have caused a pneumothorax on insertion. Search for a lung edge (and the supine deep sulcus sign) on EVERY post-insertion film before the line is used.
Self-Assessment — Confirming Safe Device Position
Use these scenarios to test whether your tubes-and-lines-first read and your adult-versus-paediatric judgement are secure under realistic pressure. Each case turns on the recurring decisions of this module — anchor each device to its correct landmark, name the specific malposition and the harm it threatens, never feed through an unconfirmed feeding tube, account for neck position when judging an endotracheal tube, and always finish with the complication search even when the device itself looks perfectly placed. For each scenario, decide both the radiological finding and the immediate clinical action before you read the discussion, exactly as you would when the film is handed to you on the unit. The accompanying table contrasts the adult and paediatric targets you should be applying, because the same systematic check must be scaled to the size of the patient.
Provided image
Scenario A: A post-subclavian-line film shows the catheter tip nicely at the cavoatrial junction, but you notice a thin lung edge at the right apex with no lung markings beyond it. The line position is perfect — is the film reassuring?
Discussion: No. A correctly positioned line can still have caused a complication. The thin apical lung edge with absent peripheral markings is a PNEUMOTHORAX from the insertion. The mandatory post-line complication check has done its job: do not use the line yet; manage the pneumothorax (observe vs chest drain by size/symptoms) and re-image. This is exactly why the complication search is non-negotiable on every post-insertion film.
Scenario B: An ET tube tip appears low on a film. You then notice the patient's chin is tucked down onto the chest. How does this change your interpretation?
Discussion: Neck FLEXION drives the ET tube tip toward the carina, so a flexed neck makes a correctly placed tube look too low ('the tube goes where the chin goes'). Re-assess the tip relative to the carina with the neck position noted; if the tube is at the right depth in neutral, no withdrawal is needed. Judging tube depth without accounting for neck position is a classic error.
Scenario C: A 2-year-old in PICU has had the ET tube repositioned. The team asks whether the adult 3–5 cm supracarinal rule applies. What do you advise?
Discussion: No — paediatric targets are age/size-specific, not the adult 3–5 cm figure, because the child's airway is short and a small migration is proportionally large; the tube also moves more with neck flexion/extension. Use the appropriate paediatric reference depth, judge against the carina with the neck noted, and re-image after the repositioning. The same systematic check applies, scaled to the child.