Page 7 of 17
RD5.3 | Emergency X-ray Interpretation in Chest, Abdomen and Skeleton — SDL Guide
Learning Objectives
- Apply a targeted emergency search pattern, overlaid on the systematic read, to a casualty chest and abdominal film.
- Recognise pneumoperitoneum (free air under the diaphragm on an erect chest film; Rigler sign on a supine abdominal film) and explain why an erect/horizontal-beam film is required.
- Identify bowel obstruction on a plain film and distinguish small-bowel from large-bowel patterns.
- Recognise an acute fracture and reliably distinguish it from a chronic/old fracture using margin, soft-tissue and healing features.
- Identify a pneumothorax (including the features of a tension pneumothorax) and state the immediate clinical action each emergency finding triggers.
INSTRUCTIONS
In casualty and the resuscitation room a plain radiograph is often the first image available, and several of its findings are time-critical: free air under the diaphragm means a perforated viscus, a tension pneumothorax can kill within minutes, and a displaced fracture needs urgent reduction. The competency RD5.3 asks you to interpret emergency conditions on the chest, abdominal and skeletal X-ray — specifically pneumoperitoneum, acute fracture, and the distinction of acute from chronic fracture. This module builds the targeted emergency read: the same disciplined search pattern you learnt for the normal film, but front-loaded to look first for the handful of findings that change management immediately, while never skipping the complete read that catches the second, unexpected injury. The recurring technical key — that free air and air–fluid levels need an erect, horizontal-beam film — runs through the whole module.
References
- Sutton's Textbook of Radiology and Imaging, 7th edition, The Acute Abdomen and Chest Emergencies (textbook)
- Grainger & Allison's Diagnostic Radiology, 7th edition, Emergency and Trauma Radiology (textbook)
- Advanced Trauma Life Support (ATLS) principles for the resuscitation-room chest radiograph (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
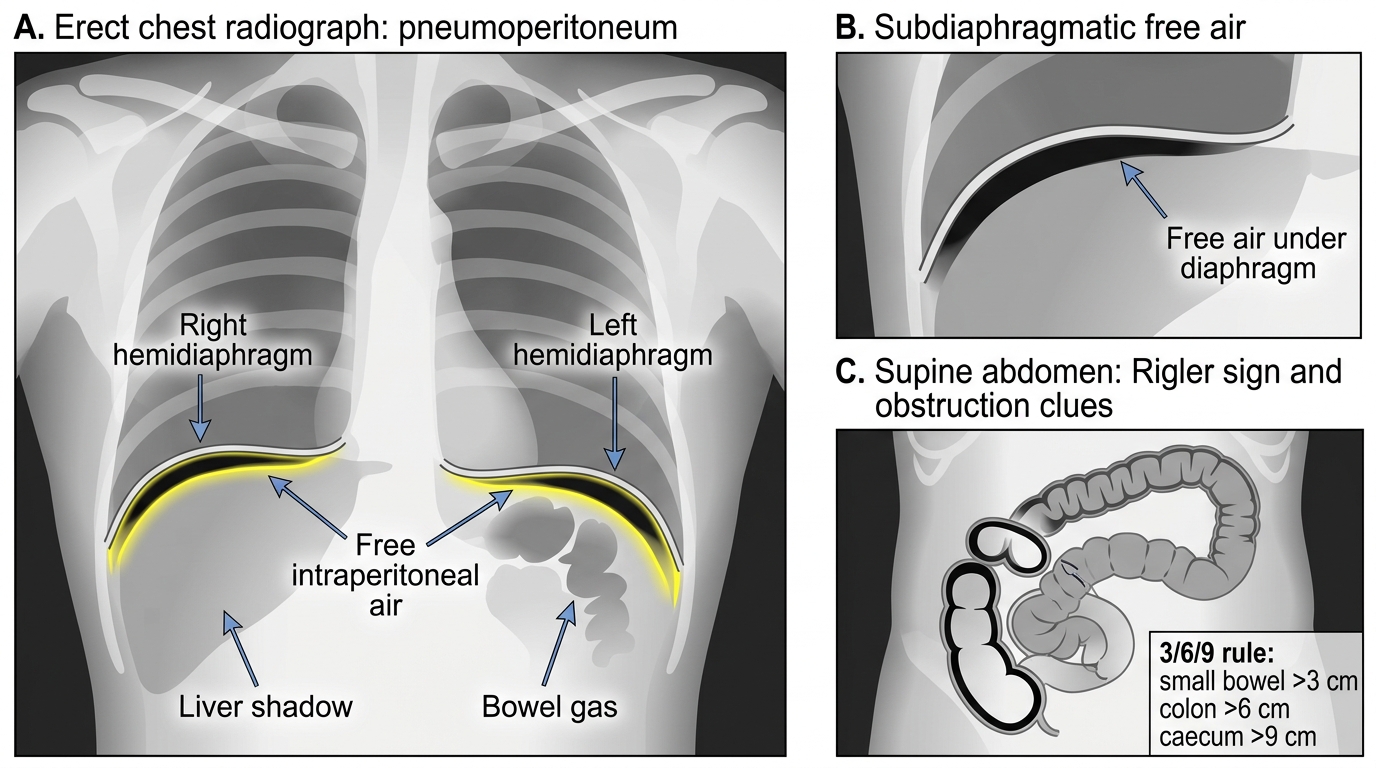
A 55-year-old man arrives in casualty doubled over with sudden severe upper-abdominal pain and a rigid, board-like abdomen. The intern, suspecting 'gastritis,' is about to send him home with antacids when the senior asks for one thing: an ERECT chest X-ray. The film shows a thin crescent of black air sitting under the right hemidiaphragm, separating it from the liver below — free intraperitoneal gas, pneumoperitoneum, the radiological signature of a perforated viscus. The 'gastritis' is a perforated peptic ulcer, and the patient is taken to theatre. Had the film been supine, the free air might have escaped notice altogether. Two decisions saved this patient: ordering the right projection, and recognising the sign. Emergency film reading is exactly this — knowing which time-critical findings to hunt for, on which projection, and acting the moment you see them. The same applies to the tension pneumothorax that shifts a mediastinum and to the displaced fracture that must be reduced tonight.
WHY THIS MATTERS
Every doctor who works a casualty shift will read emergency radiographs before the formal report exists, and some of those findings cannot wait. The NMC competency RD5.3 names the highest-stakes examples explicitly — pneumoperitoneum, acute fracture, and the distinction between an acute and a chronic fracture — because each carries an immediate management consequence and each is a classic missed diagnosis. Missing free air under the diaphragm delays surgery for a perforation, with rising mortality by the hour; missing a tension pneumothorax can be rapidly fatal; misreading an old, healed fracture as a fresh injury sends a patient for needless immobilisation, while missing a genuinely acute fracture risks displacement, non-union and nerve or vessel injury. The skill is not new knowledge so much as disciplined application under pressure: the same search pattern from the normal film, but with a deliberate first pass for the life- and limb-threatening signs, and an unshakeable habit of confirming the projection (erect for free air and fluid levels) before committing. This is daily, examinable, and squarely a patient-safety competency for the generalist, not the radiologist alone.
RECALL
Before reading further, recall the foundations this emergency skill builds on:
- The normal template and search pattern (RD5.1): the normal chest, abdominal and skeletal film — free air, dilated bowel and a fracture line are all DEVIATIONS from that learnt normal, so the normal template is the detector.
- Radiographic densities: air is the blackest density; free intraperitoneal gas is therefore a black collection where soft tissue/water should be, e.g. under the diaphragm or outlining a bowel wall.
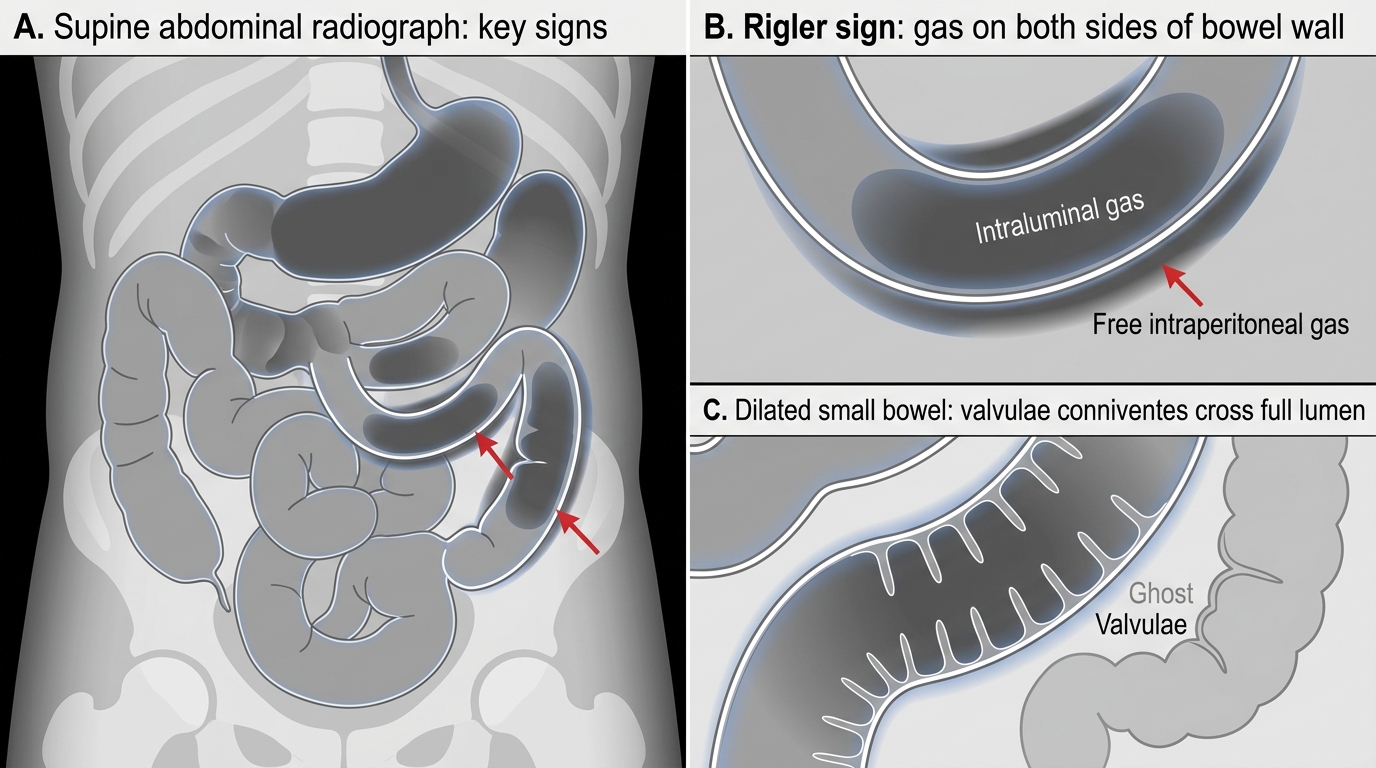
- Bowel anatomy: small-bowel valvulae conniventes cross the FULL width of the lumen; large-bowel haustra do NOT — the key to localising an obstruction.
- Normal cortex and corticated margins (RD5.1): a normal bone cortex is smooth and continuous; a fresh fracture breaks it with a sharp non-corticated lucent line, whereas an old fracture has had time to develop sclerotic, corticated (healed) margins.
- Projection physics: free air rises and air–fluid levels form a horizontal interface only on an ERECT (horizontal-beam) film — a supine film can hide both.
If the normal bowel pattern or the cortex concept is hazy, a quick review of RD5.1 now will make the emergency signs below far easier to spot.
Why Rapid, Reliable Emergency Film Reading Saves Lives
Emergency radiograph interpretation differs from routine reading in one respect that matters enormously: a subset of findings must be recognised and acted upon within minutes, not at the leisure of a formal report. In casualty and the resuscitation room the plain film is frequently the first and fastest image available, and the clinician at the bedside is often the first — and sometimes the only — person to look at it. The competency RD5.3 deliberately names the findings whose miss is most catastrophic: pneumoperitoneum (free air signalling a perforated viscus), acute fracture, and the acute-versus-chronic fracture distinction; to these the same emergency read adds the tension pneumothorax and bowel obstruction. The unifying clinical truth is that each of these findings has an immediate action attached to it, so detection and decision are coupled.
The stakes are concrete and time-dependent:
Time-Critical Plain-Film Findings in Casualty
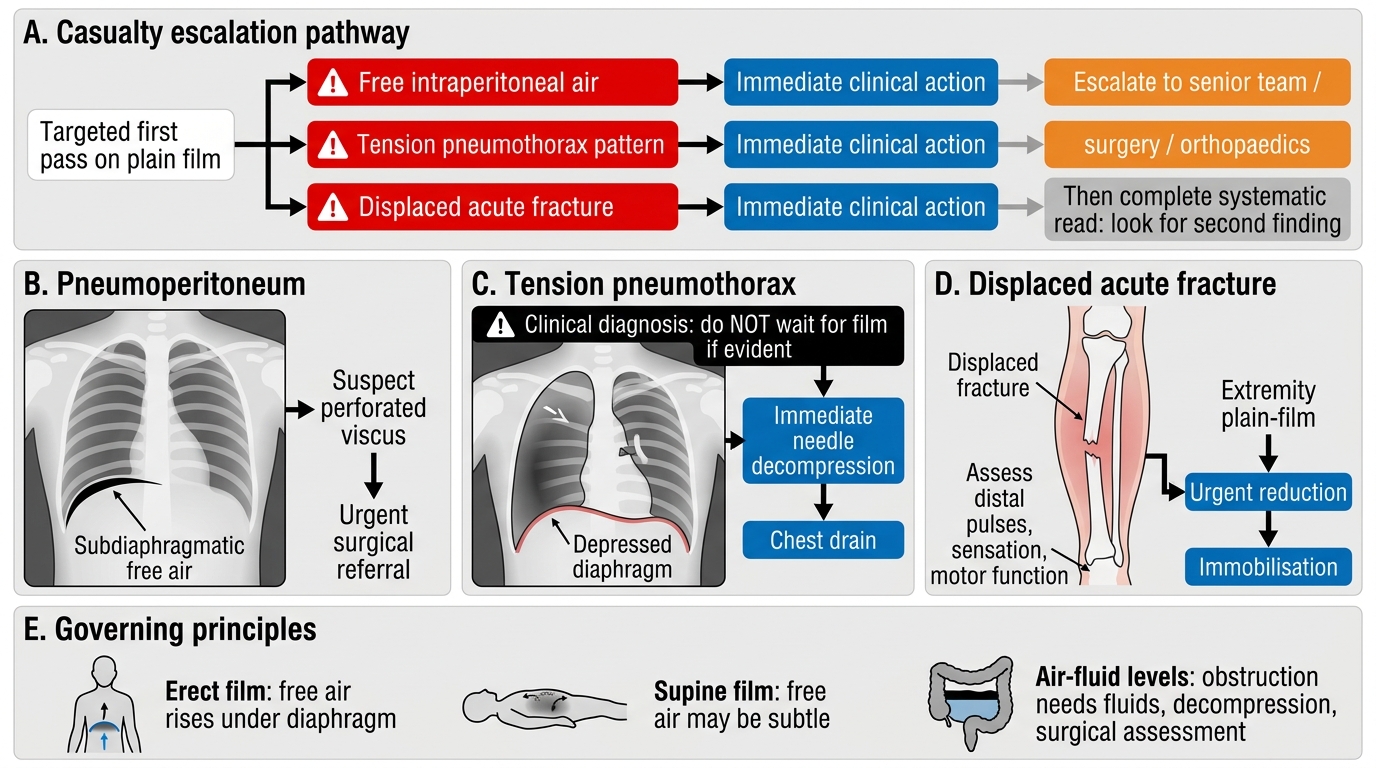
- Pneumoperitoneum → suspect a perforated viscus → urgent surgical referral; delay raises mortality hour by hour.
- Tension pneumothorax → mediastinal shift away from the affected side → immediate needle decompression then chest drain; this is a CLINICAL diagnosis, and if clinically evident you must NOT wait for a film.
- Displaced/acute fracture → urgent reduction and immobilisation; assess for neurovascular injury.
- Bowel obstruction → fluid resuscitation, decompression, surgical assessment.
The discipline that makes this reliable is a targeted first pass for these life- and limb-threatening signs, followed — never replaced — by the complete systematic read that catches the second, unexpected finding.
Governing Principles — Erect Films, Free Air, Air–Fluid Levels and the Targeted Search
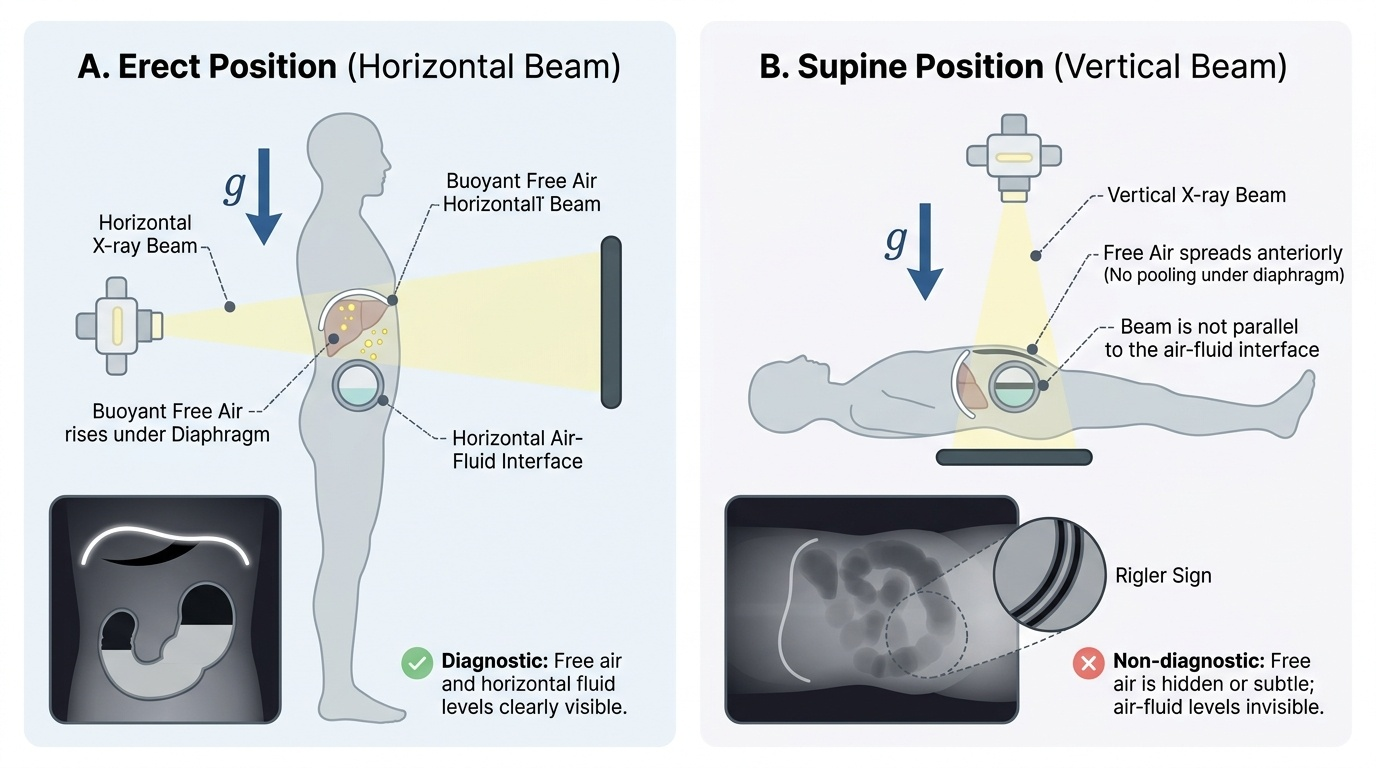
Three governing principles make emergency interpretation reliable, and the first is so important it deserves to become a reflex: the PROJECTION determines whether the emergency sign is even visible. Free intraperitoneal gas is buoyant — it rises to the highest point. On an ERECT chest or abdominal film, with the patient upright for several minutes, that gas collects UNDER the diaphragm and is seen as a thin black crescent separating the diaphragm from the liver or stomach. On a SUPINE film the gas spreads over the anterior abdomen and may be invisible or show only subtle signs (the Rigler/double-wall sign). Likewise, air–fluid levels — the hallmark of obstruction and of an abscess or hydropneumothorax — form a flat horizontal interface only when the X-ray beam is HORIZONTAL (erect or lateral decubitus). A supine film, with a vertical beam, cannot demonstrate a fluid level. Therefore the right projection (erect CXR, or a left-lateral decubitus if the patient cannot stand) must be requested and confirmed before you conclude there is no free air.
The second principle is that the emergency signs are simply density deviations from the normal template:
Provided image
- Free gas = black (air density) where soft tissue should be — under the diaphragm, or outlining the OUTER wall of bowel (Rigler sign).
- A fracture = a black (lucent) line breaking the white cortex, often with soft-tissue swelling.
- Obstruction = abnormally dilated, gas-filled loops with air–fluid levels on the erect film.
The third principle is the targeted-then-systematic search: scan first for the handful of killers, then complete the full normal-template read so a second finding is never missed.
SELF-CHECK
A patient with severe abdominal pain has a SUPINE abdominal radiograph that shows no obvious free air, but you remain clinically concerned about a perforation. What is the most appropriate next imaging step?
A. Accept the supine film as excluding free air and reassure the patient
B. Obtain an ERECT chest X-ray (or a left-lateral decubitus film if the patient cannot stand) to demonstrate free air under the diaphragm
C. Repeat the same supine abdominal film
D. Order an MRI abdomen to look for free air
Reveal Answer
Answer: B. Obtain an ERECT chest X-ray (or a left-lateral decubitus film if the patient cannot stand) to demonstrate free air under the diaphragm
Free intraperitoneal gas rises to the highest point and is best shown UNDER the diaphragm on an ERECT chest film, with the patient upright for several minutes; a left-lateral decubitus film is the alternative if the patient cannot stand. A supine film can miss free air (look for the Rigler/double-wall sign as a subtle clue but it is not sensitive), so a negative supine film does not exclude perforation. Repeating the supine film adds nothing, and MRI is not the appropriate tool for acute free air.
Method — Searching the Emergency Chest, Abdomen and Skeleton for Time-Critical Signs
The emergency method is the systematic read with a targeted first pass for the killers, applied region by region. As always, begin by confirming identity, date and PROJECTION — an erect chest film if free air or a fluid level is a possibility. Then run the emergency search before the leisurely complete read, because the findings below change management at once. The point is not to abandon the full read but to front-load the time-critical hunt onto the same disciplined sequence you already know.
Emergency chest (erect CXR): look first for a PNEUMOTHORAX — a lung edge (visceral pleural line) with absent lung markings peripheral to it; in a TENSION pneumothorax the mediastinum is shifted AWAY from the affected side and the hemidiaphragm is depressed (a clinical emergency — act, do not wait). Then look for FREE AIR under the diaphragm (pneumoperitoneum), a large effusion/haemothorax (meniscus or whole-hemithorax white-out), lobar collapse, and a widened mediastinum.
Pneumoperitoneum and Emergency Abdominal Free Air Signs
Emergency abdomen (supine ± erect/decubitus): scan for free air signs on the supine film — the Rigler (double-wall) sign, where gas outlines BOTH the inner and outer walls of a bowel loop because there is gas inside the bowel and free gas outside it — and for bowel OBSTRUCTION: abnormally dilated gas-filled loops, and air–fluid levels on the erect film. Apply the calibre 3/6/9 rule (small bowel >~3 cm, large bowel >~6 cm, caecum >~9 cm).
Rigler Sign and Dilated Small Bowel on Supine Abdominal Radiograph
Emergency skeleton (always TWO orthogonal views): read alignment (dislocation, angulation), then the cortex for a break (a sharp lucent line or a step/buckle in the cortex), then the joint, then the SOFT TISSUES — soft-tissue swelling, a joint effusion (e.g. the elbow fat-pad sign), or surgical emphysema are vital clues that point to an underlying acute fracture even when the line is subtle. A single view can hide a fracture or dislocation, so two orthogonal views are mandatory.