Page 8 of 17
RD5.3 | Emergency X-ray Interpretation in Chest, Abdomen and Skeleton — SDL Guide (Part 2)
Interpreting the Findings — Pneumoperitoneum, Obstruction and Acute vs Chronic Fracture
Having detected an emergency sign, the interpretive task is to confirm it, characterise it, and distinguish it from its mimics — and for fractures specifically, to judge whether it is ACUTE or OLD, which the competency calls out by name. For pneumoperitoneum, confirm free air under the diaphragm on the erect film and the Rigler sign on the supine film, and exclude the classic mimics: the Chilaiditi sign (colon interposed between liver and diaphragm — note the haustral folds within the gas, which true free air lacks) and the normal gastric air bubble under the LEFT hemidiaphragm. For obstruction, decide the LEVEL — small-bowel versus large-bowel — because it changes the differential and the management.
Provided image
The small- versus large-bowel distinction rests on position and mucosal pattern:
Provided image
| Feature | Small-bowel obstruction | Large-bowel obstruction |
|---|---|---|
| Location of loops | Central | Peripheral (frames the abdomen) |
| Mucosal markings | Valvulae conniventes cross the FULL lumen | Haustra do NOT cross the full lumen |
| Calibre threshold | >~3 cm | >~6 cm (caecum >~9 cm) |
| Air–fluid levels | Multiple, central, 'stepladder' | Fewer, peripheral |
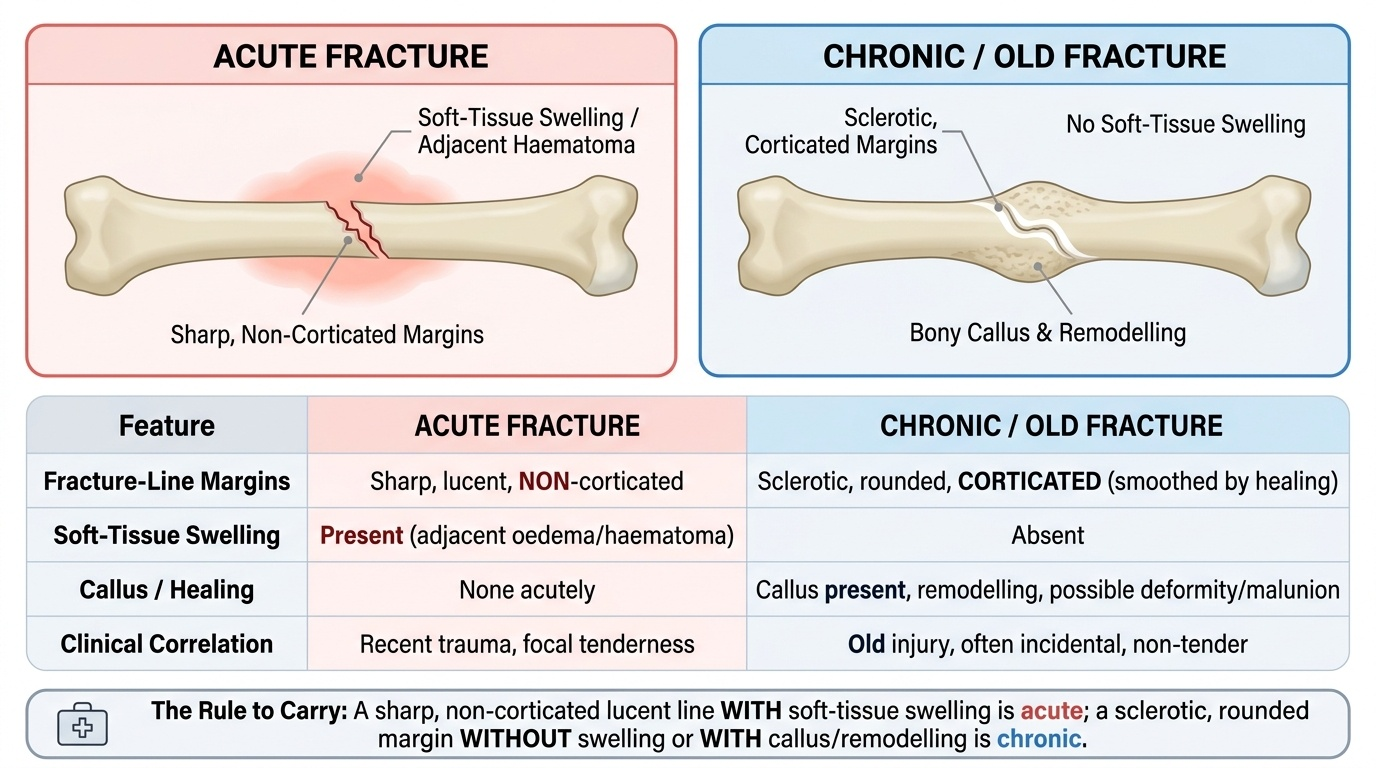
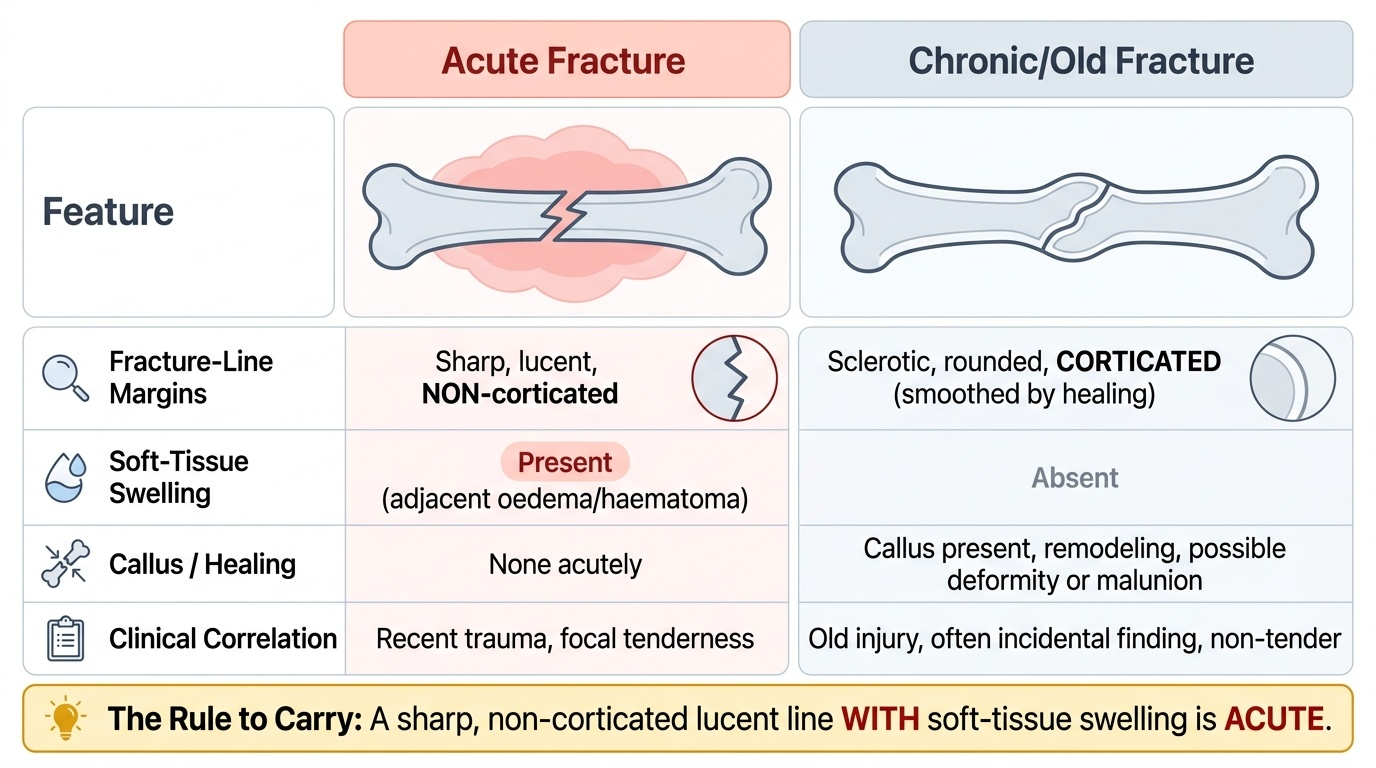
The acute-versus-chronic fracture distinction is a high-yield, named part of the competency and turns on three discriminators — margins, soft tissue, and healing:
| Feature | Acute fracture | Chronic / old fracture |
|---|---|---|
| Fracture-line margins | Sharp, lucent, NON-corticated | Sclerotic, rounded, CORTICATED (smoothed by healing) |
| Soft-tissue swelling | Present (adjacent oedema/haematoma) | Absent |
| Callus / healing | None acutely | Callus, remodelling, possible deformity/malunion |
| Clinical correlation | Recent trauma, focal tenderness | Old injury, often incidental, non-tender |
The rule to carry: a sharp non-corticated lucent line WITH soft-tissue swelling is acute; a sclerotic, rounded, corticated margin WITHOUT swelling is old. When uncertain, correlate clinically and compare with any prior films.
Applied Practice — Working Through Emergency Films Under Time Pressure
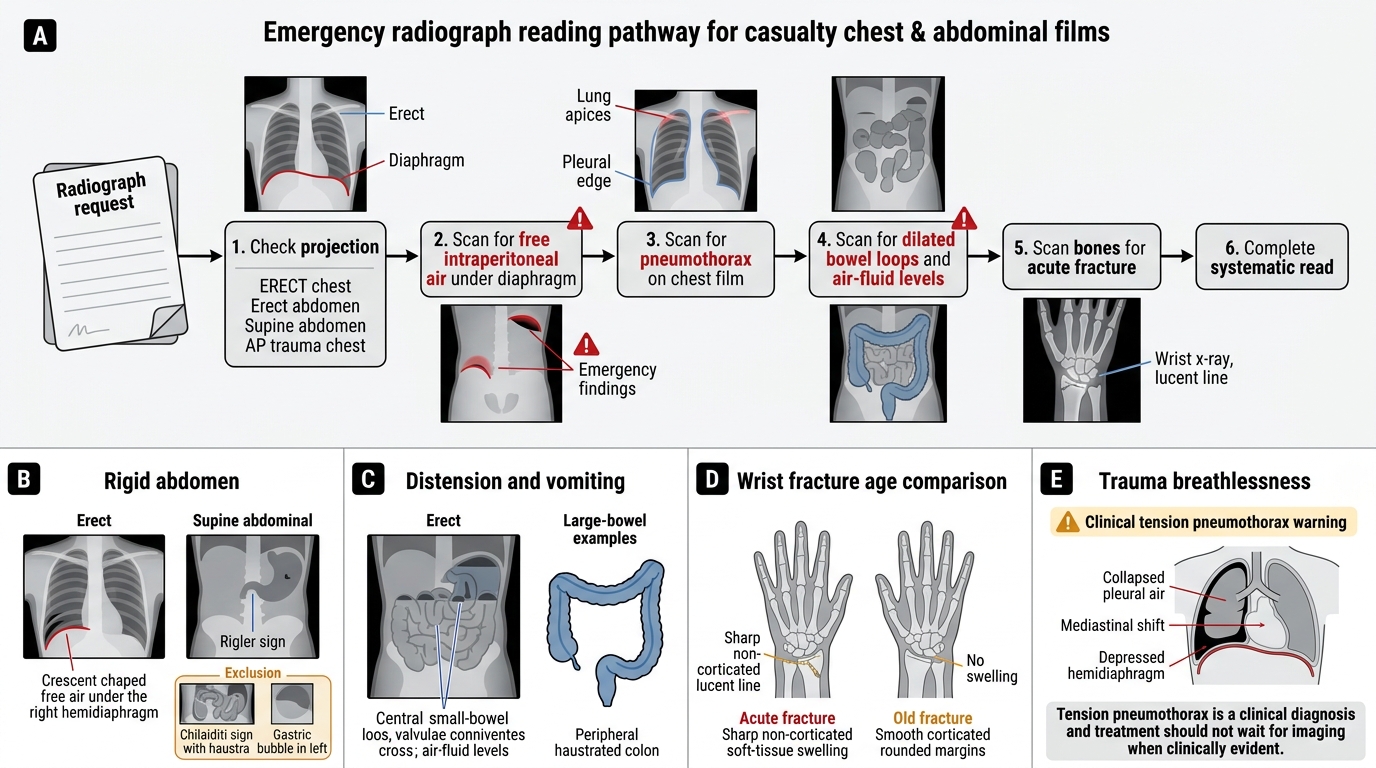
Applied practice means running the targeted-then-systematic read on real casualty films and coupling each finding to its action, because in an emergency a finding that is detected but not acted upon is clinically useless. Rehearse the four-step sequence below until it is automatic: first confirm the projection (is this an erect, horizontal-beam film if free air or a fluid level is possible?); second, sweep deliberately for the killers — pneumothorax, free air under the diaphragm, abnormally dilated bowel, and an acute fracture; third, complete the full systematic read so that no second, unexpected finding is missed; and fourth, act on what you found, escalating immediately for the life- and limb-threatening signs. The worked cases that follow show how this single discipline applies across the chest, the abdomen and the skeleton, and how the same projection check and targeted first pass turn a slow, error-prone read into a fast and safe one.
Targeted Emergency Read of Chest and Abdominal Films
Worked case 1 — the rigid abdomen (the hook): sudden severe abdominal pain, board-like abdomen. ACTION: request an ERECT chest film; look for free air under the diaphragm; if present, treat as a perforated viscus and refer surgically urgently. Confirm with the Rigler sign on the supine film and exclude Chilaiditi (haustra within the gas) and the gastric bubble (left side).
Worked case 2 — distension and vomiting: a distended abdomen with vomiting and absolute constipation. ACTION: look for dilated loops and air–fluid levels on the erect film; decide small- vs large-bowel by central/peripheral position and valvulae-vs-haustra; resuscitate, decompress, and obtain surgical assessment.
Worked case 3 — wrist injury, but is it new?: a patient with wrist pain and a lucent line on the film. ACTION: apply the acute-vs-chronic discriminators — sharp non-corticated margins plus soft-tissue swelling means ACUTE (immobilise, assess neurovascular status, two views); sclerotic, corticated, rounded margins without swelling means an OLD fracture (no acute action, correlate clinically).
Worked case 4 — breathless after trauma: sudden breathlessness with absent breath sounds on one side. The key teaching point: a TENSION pneumothorax is a CLINICAL diagnosis — if it is clinically evident (tracheal deviation, hypotension, absent breath sounds) decompress IMMEDIATELY and do not wait for the radiograph. If imaged, expect a lung edge with absent peripheral markings and mediastinal shift AWAY from the affected side. The cross-cutting applied lesson is that the projection check and the targeted first pass turn a slow, error-prone read into a fast, safe one.
SELF-CHECK
A radiograph of the forearm in a patient with a vague history of old trauma shows a transverse line across the ulna. The line has sclerotic, rounded, corticated margins, there is no surrounding soft-tissue swelling, and the patient is non-tender over the site. How should this be interpreted?
A. An acute fracture requiring urgent immobilisation
B. An old (chronic/healed) fracture — sclerotic corticated rounded margins and absent soft-tissue swelling indicate it is not recent
C. Osteomyelitis
D. A tension pneumothorax
Reveal Answer
Answer: B. An old (chronic/healed) fracture — sclerotic corticated rounded margins and absent soft-tissue swelling indicate it is not recent
The discriminators of an OLD fracture are sclerotic, rounded, CORTICATED margins (the line has been smoothed by healing/remodelling) and the ABSENCE of soft-tissue swelling, usually with no acute clinical tenderness. An acute fracture has a sharp, NON-corticated lucent line WITH adjacent soft-tissue swelling and recent-trauma tenderness. These features mark this as an old fracture, so no acute immobilisation is needed — correlate clinically and with any prior films.
SELF-CHECK
On an erect abdominal film, dilated bowel loops are seen in the CENTRE of the abdomen, with mucosal folds that cross the FULL width of the lumen, and multiple central air–fluid levels in a stepladder pattern. What does this most likely represent?
A. Large-bowel obstruction
B. Small-bowel obstruction
C. Normal bowel gas pattern
D. Pneumoperitoneum
Reveal Answer
Answer: B. Small-bowel obstruction
Centrally located dilated loops with valvulae conniventes that cross the FULL width of the lumen, and multiple central 'stepladder' air–fluid levels, are the classic plain-film features of SMALL-bowel obstruction. Large-bowel obstruction shows peripherally located loops with haustra that do NOT cross the full lumen and fewer, peripheral levels. The pattern is clearly abnormal (dilatation + fluid levels), excluding a normal gas pattern, and there is no free air described to suggest pneumoperitoneum.
CLINICAL PEARL
Pearl 1 — Confirm the projection before excluding free air. Free intraperitoneal gas and air–fluid levels need an ERECT (horizontal-beam) film; a supine film can hide both. A negative supine abdominal film does NOT exclude a perforation — get an erect CXR (or left-lateral decubitus).
Pearl 2 — Soft tissues are the fracture's tell-tale. When a bony injury is subtle, soft-tissue swelling, a joint effusion (e.g. the elbow fat-pad sign) or surgical emphysema points you to the acute fracture. Always read the soft tissues, and always get TWO orthogonal views.
Pearl 3 — Tension pneumothorax is a CLINICAL diagnosis. If clinically evident (tracheal deviation, hypotension, absent breath sounds), decompress immediately — do NOT wait for the X-ray. The film, if obtained, shows a lung edge with absent peripheral markings and mediastinal shift AWAY from the affected side.
Self-Assessment — Recognising the Emergency Sign
Use these scenarios to test your emergency recognition and the action each finding triggers. The cases deliberately revisit the recurring decisions of this module — confirm the projection, distinguish a real emergency sign from its mimic, and separate an acute from an old fracture — so work through each one, decide on both the finding and the immediate action, and only then read the discussion. As in casualty, naming the sign is only half the task; the management response is the other half.
Scenario A: A supine abdominal film in a patient with peritonism shows gas outlining both the inner and the outer wall of a loop of bowel. What is the sign, what does it indicate, and what do you do?
Discussion: This is the Rigler (double-wall) sign — gas inside the bowel AND free gas outside it both outline the wall — indicating pneumoperitoneum from a perforated viscus. Confirm with an erect chest film (free air under the diaphragm) and refer surgically urgently. Exclude the Chilaiditi mimic (interposed colon shows haustral folds within the gas).
Scenario B: A casualty officer is about to send a breathless trauma patient for a chest X-ray. The patient has a deviated trachea, distended neck veins, hypotension and absent breath sounds on the right. What is the priority?
Discussion: This is a clinically evident TENSION pneumothorax — a clinical diagnosis. The priority is IMMEDIATE needle decompression followed by a chest drain; do NOT wait for the radiograph. Imaging would only confirm the lung edge and mediastinal shift away from the affected side, and the delay could be fatal.
Scenario C: Two patients each have a lucent line across a metacarpal. In the first the line is sharp and non-corticated with overlying soft-tissue swelling; in the second the line is sclerotic, rounded and corticated with no swelling. How do you classify each?
Discussion: The first is an ACUTE fracture (sharp non-corticated margins + soft-tissue swelling) — immobilise, assess neurovascular status, two views. The second is an OLD/healed fracture (sclerotic corticated rounded margins, no swelling) — no acute intervention; correlate clinically. This is exactly the acute-versus-chronic discrimination the competency requires.