Page 4 of 17
RD7.1 | Imaging in Ectopic Pregnancy — SDL Guide
Learning Objectives
- State the clinical indications for urgent imaging in a woman of reproductive age with a positive pregnancy test, abdominal pain and/or bleeding.
- Justify transvaginal ultrasound as the first-line imaging modality and explain its partnership with serum beta-hCG and the discriminatory zone.
- Describe the expected ultrasound findings of tubal ectopic pregnancy and the danger of assuming an intrauterine pregnancy that has not been seen.
- Integrate the ultrasound findings and the beta-hCG level into the diagnosis, including the concept of pregnancy of unknown location and the heterotopic trap.
- Integrate the imaging findings into management decisions, distinguishing the haemodynamically stable from the unstable patient.
INSTRUCTIONS
Ectopic pregnancy is the leading cause of maternal death in the first trimester and a true emergency that every clinician must be able to suspect, investigate and escalate. The diagnosis hinges on the intelligent combination of two tests — transvaginal ultrasound and serum beta-hCG — neither of which is sufficient alone. As a final-year student you will meet women with early-pregnancy pain and bleeding in casualty, gynaecology and family medicine, and the imaging decisions made in the first hour can be the difference between a planned treatment and a ruptured tube with haemorrhagic shock. This module teaches you how to choose the imaging, how to read it alongside the hormone level, and the cardinal safety rule: never assume an intrauterine pregnancy you have not actually seen.
References
- Sutton's Textbook of Radiology and Imaging, 7th edition, Chapter on Obstetric and Gynaecological Ultrasound (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter on Early Pregnancy Imaging (textbook)
- NICE NG126 / RCOG Green-top Guideline No. 21 — Diagnosis and Management of Ectopic Pregnancy and Miscarriage (guideline)
- DC Dutta's Textbook of Obstetrics, Chapter on Ectopic Pregnancy (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 27-year-old woman arrives in casualty with six weeks of amenorrhoea, lower abdominal pain and a little vaginal spotting. Her urine pregnancy test is positive. She is pale but her blood pressure is, for now, normal. The casualty officer faces a decision that cannot be deferred: is this a normal early intrauterine pregnancy, a miscarriage, or an ectopic pregnancy quietly stretching a fallopian tube towards rupture? The wrong assumption here is lethal. If the team reassures her that 'the pregnancy test is positive so it's probably fine' and sends her home, a tubal rupture overnight can fill her abdomen with blood. The right move is a transvaginal ultrasound read together with a serum beta-hCG — and a discipline that refuses to call any pregnancy intrauterine until it has actually been seen inside the uterus.
WHY THIS MATTERS
Ectopic pregnancy complicates roughly 1-2% of pregnancies and remains the commonest cause of maternal death in the first trimester, almost always from haemorrhage following tubal rupture. Early diagnosis — before rupture — transforms a life-threatening emergency into a condition that can often be managed medically or even expectantly. The NMC competency RD7.1 requires you to integrate provided imaging findings into the management of ectopic pregnancy, and this is one of the clearest examples in all of medicine of imaging plus a biochemical test driving an immediate, potentially life-saving decision. You will encounter early-pregnancy pain and bleeding in every acute clinical posting; knowing how transvaginal ultrasound and serum beta-hCG fit together, and the safety rules that govern their interpretation, is core clinical competence rather than specialist knowledge.
RECALL
Before reading further, recall:
- Tubal anatomy and implantation (from AN/OG): fertilisation normally occurs in the ampulla of the fallopian tube, and the conceptus then travels to implant in the uterine cavity. If transport is delayed or obstructed (e.g. by prior pelvic inflammatory disease, tubal surgery or an intrauterine device in situ), the conceptus implants outside the cavity — most often in the ampullary part of the tube, the commonest ectopic site.
- Beta-hCG physiology (from PY/OG): human chorionic gonadotrophin is secreted by trophoblast; in a normal early intrauterine pregnancy its serum level roughly doubles every 48 hours (a rise of about 35-66% over 48 h is reassuring). The level reflects trophoblastic mass, not location — so a positive or rising hCG does NOT prove the pregnancy is in the uterus.
- Normal early ultrasound milestones: with transvaginal scanning, an intrauterine gestational sac is usually first seen around 5 weeks, a yolk sac shortly after, and a fetal pole with cardiac activity by about 6 weeks. These milestones underpin the discriminatory-zone concept.
- Ultrasound safety: ultrasound uses no ionising radiation and is the imaging workhorse of early pregnancy; the transvaginal approach places a high-frequency probe close to the uterus and adnexa, giving the resolution needed to localise an early pregnancy.
Clinical Scenario — Early Pregnancy with Pain and Bleeding: The Question That Must Be Answered
The clinical scenario in which imaging is requested for suspected ectopic pregnancy is one of the most important to recognise in acute care: any woman of reproductive age with a positive pregnancy test and abdominal or pelvic pain, with or without vaginal bleeding, has an ectopic pregnancy until proven otherwise. The presentation ranges from the classic triad of amenorrhoea, pain and bleeding to subtle or atypical complaints such as shoulder-tip pain (diaphragmatic irritation from haemoperitoneum), dizziness or syncope, or simply unexplained early-pregnancy pain. Because the consequences of a missed diagnosis are catastrophic, the threshold to investigate is deliberately low, and the single most important first action is to establish that the woman is pregnant and then to localise that pregnancy. This is the focused question imaging exists to answer in this scenario: where is the pregnancy?
The risk factors that raise the prior probability of an ectopic pregnancy, and should heighten suspicion, include:
- Previous ectopic pregnancy (the strongest single risk factor).
- Prior pelvic inflammatory disease or tubal infection (e.g. chlamydia), and previous tubal surgery.
- Assisted reproduction (IVF), which also raises the rare risk of a heterotopic pregnancy.
- An intrauterine contraceptive device in situ or progestogen-only contraception, and a history of subfertility.
The clinical state of the patient frames the urgency. A haemodynamically unstable woman — tachycardia, hypotension, signs of peritonism — needs immediate resuscitation and is likely to proceed to emergency surgery on clinical grounds, with imaging used only insofar as it does not delay theatre. A stable woman is investigated systematically with transvaginal ultrasound and serum beta-hCG, which together localise the pregnancy and guide management. Recognising which of these two situations you are in is the first decision in the pathway.
Imaging Strategy — Transvaginal Ultrasound Plus the Discriminatory Zone
The imaging strategy for suspected ectopic pregnancy rests on a partnership between one imaging test and one biochemical test, because neither answers the question alone. Transvaginal ultrasound localises the pregnancy when it can be seen, but in very early pregnancy nothing may yet be visible; serum beta-hCG tells you how advanced the pregnancy is and therefore whether an intrauterine pregnancy SHOULD be visible by now. Interpreting the two together — the ultrasound finding against the hCG level — is the core diagnostic skill, and the framework that links them is the discriminatory zone. As always in early pregnancy, ultrasound is chosen because it uses no ionising radiation and the transvaginal route gives the high resolution required to identify a small early gestation in the uterus or adnexa.
Transvaginal ultrasound (TVS) — first-line imaging:
The high-frequency endovaginal probe images the uterus and adnexa at close range, allowing detection of an intrauterine gestational sac, a yolk sac, a fetal pole, or an adnexal ectopic mass. It is the first-line and definitive imaging modality for localising an early pregnancy. Transabdominal ultrasound (TAS) is only an adjunct, useful for an overview or when the patient declines TVS or has a large haemoperitoneum, but its lower resolution makes it unreliable for confidently localising an early gestation.
Serum beta-hCG and the discriminatory zone:
The discriminatory zone is the serum beta-hCG level above which an intrauterine gestational sac should normally be visible on transvaginal ultrasound if the pregnancy is intrauterine — conventionally taken as approximately 1500-2000 IU/L. The logic is decisive: if the beta-hCG is ABOVE the discriminatory zone but the uterus is EMPTY on a good-quality transvaginal scan, the pregnancy is highly likely to be ectopic (or a non-viable intrauterine pregnancy). When the beta-hCG is BELOW the discriminatory zone and the scan is inconclusive, a single scan cannot exclude either a very early intrauterine pregnancy or an ectopic, and the situation is classified as a pregnancy of unknown location pending serial assessment.
A single threshold must be applied with care: the discriminatory zone is higher in multiple pregnancy (more trophoblast for a given gestation), and modern guidance (NICE/RCOG) stresses serial beta-hCG measurement combined with repeat TVS rather than acting on a single hCG value, to avoid wrongly interrupting a potentially viable early intrauterine pregnancy. A normal viable intrauterine pregnancy typically shows roughly a 35-66% rise in beta-hCG over 48 hours, whereas a suboptimal rise or a plateau raises suspicion of an ectopic or a failing pregnancy.
MRI is reserved for rare problem-solving — for example, characterising a suspected interstitial or caesarean-scar ectopic when ultrasound is inconclusive — and uses no ionising radiation. CT has no role in the elective diagnostic pathway; it would only feature incidentally in an unstable, undifferentiated acute abdomen, and even then ultrasound and clinical assessment lead in a pregnant woman.
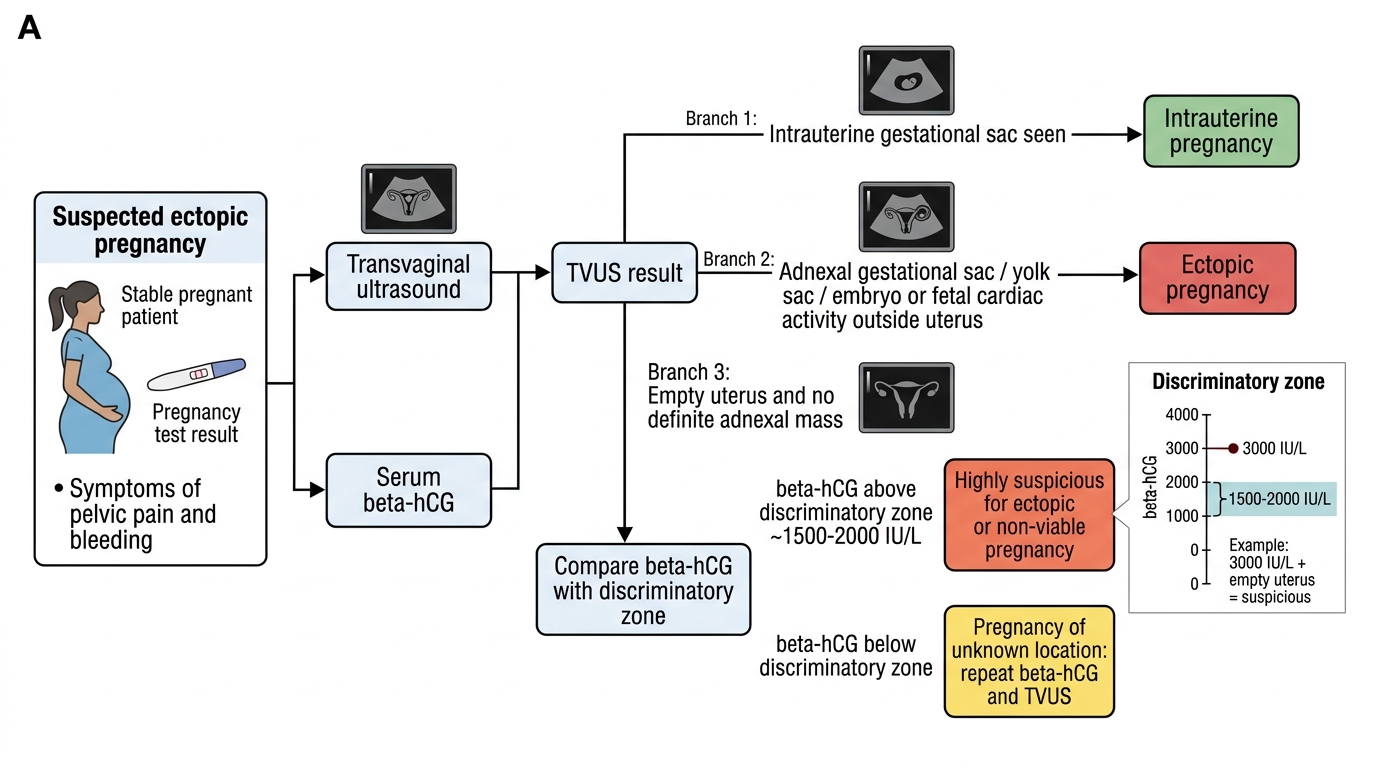
TVUS and beta-hCG Decision Flow for Suspected Ectopic Pregnancy
SELF-CHECK
A stable woman with 6 weeks of amenorrhoea and a positive pregnancy test has a serum beta-hCG of 3000 IU/L. A good-quality transvaginal ultrasound shows an empty uterus and no definite adnexal mass. How should this combination be interpreted?
A. Reassuring — the high beta-hCG confirms a healthy intrauterine pregnancy that is simply too small to see
B. Highly suspicious for ectopic (or non-viable) pregnancy, because the beta-hCG is above the discriminatory zone (~1500-2000 IU/L) yet the uterus is empty
C. Definitely a complete miscarriage; no further action is needed
D. Normal — an empty uterus at any beta-hCG level is expected at 6 weeks
Reveal Answer
Answer: B. Highly suspicious for ectopic (or non-viable) pregnancy, because the beta-hCG is above the discriminatory zone (~1500-2000 IU/L) yet the uterus is empty
A beta-hCG of 3000 IU/L is above the transvaginal discriminatory zone (~1500-2000 IU/L), at which an intrauterine gestational sac should be visible if the pregnancy is intrauterine. An EMPTY uterus at this level is highly suspicious for an ectopic pregnancy or a non-viable intrauterine pregnancy, and the patient must be managed accordingly (close observation, possible diagnostic/therapeutic intervention), not reassured. A high beta-hCG reflects trophoblastic mass, not location.
Expected Imaging Findings — From Empty Uterus to Tubal Ring and Free Fluid
Recognising the ultrasound findings of ectopic pregnancy, and understanding what their absence does and does not mean, is the interpretive heart of this topic. The single most important principle is also the safest: an intrauterine pregnancy is only confirmed when an intrauterine gestational sac containing a yolk sac or fetal pole is actually SEEN within the uterine cavity. An empty uterus does not exclude pregnancy, and an apparent 'sac-like' structure in the uterus can be a deceptive pseudosac. Because the management of an ectopic and an intrauterine pregnancy are diametrically opposite, the radiological distinction is not academic — it determines whether the patient is treated for an ectopic or reassured. Reading the findings against the beta-hCG level, as set out above, is what makes them meaningful.
The ultrasound findings that point to a tubal ectopic pregnancy are:
- Empty uterus in the presence of a positive pregnancy test and a beta-hCG above the discriminatory zone — the key indirect sign.
- Adnexal 'tubal ring' (bagel/donut) mass: an echogenic ring with a hypoechoic centre in the adnexa, lying SEPARATE from the ovary — a highly specific direct sign of a tubal ectopic. Sometimes a yolk sac, fetal pole or even cardiac activity is seen within this extrauterine mass (definitive).
- Free fluid in the pouch of Douglas: simple anechoic fluid may be physiological, but echogenic free fluid (suggesting blood) raises concern for tubal leakage or rupture and is an important warning sign.
- Pseudogestational sac: a fluid collection centrally within the endometrial cavity, sometimes seen with ectopic pregnancy, that mimics a true intrauterine sac. Unlike a true gestational sac it lies centrally (not eccentrically implanted), lacks the double decidual sign, and contains no yolk sac — do NOT mistake it for an intrauterine pregnancy.
Two further points complete the picture. First, never assume an intrauterine pregnancy you have not seen: a positive test with an empty uterus is a pregnancy of unknown location until proven otherwise, not a reassuring intrauterine pregnancy. Second, non-tubal ectopic sites have characteristic appearances — an interstitial (cornual) ectopic sits high in the cornu with a thin surrounding myometrial mantle and can bleed catastrophically; a caesarean-scar ectopic implants in the lower-segment scar; a cervical ectopic sits within the cervix. These rarer sites are where MRI occasionally helps when TVS is inconclusive.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
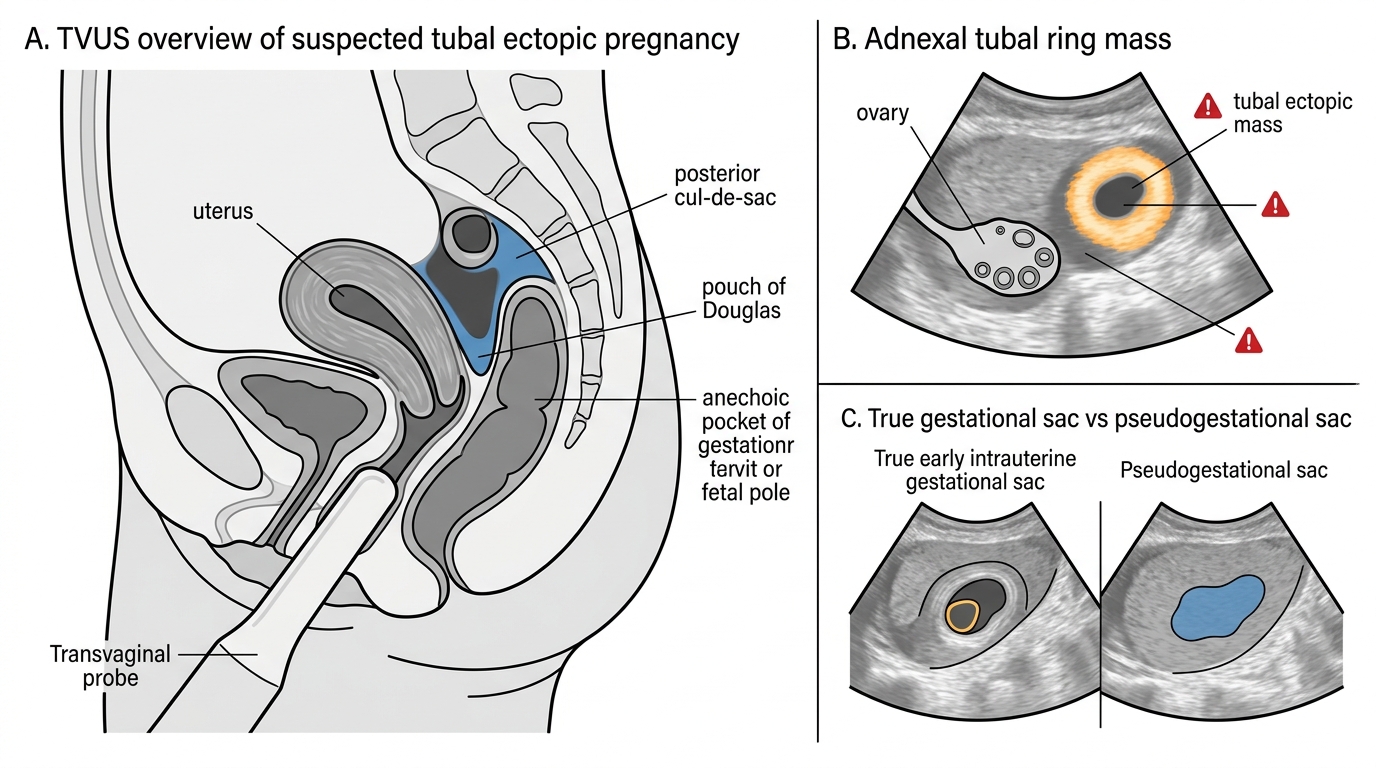
Transvaginal Ultrasound Features of Tubal Ectopic Pregnancy
SELF-CHECK
On transvaginal ultrasound of a woman with a positive pregnancy test, a central fluid collection is seen within the endometrial cavity. Which feature would tell you this is a PSEUDOGESTATIONAL sac rather than a true early intrauterine gestational sac?
A. It lies eccentrically within the endometrium and shows a double decidual sign
B. It contains a clearly visible yolk sac
C. It lies centrally within the cavity, lacks a double decidual sign and contains no yolk sac
D. It is surrounded by a thick echogenic trophoblastic ring with cardiac activity
Reveal Answer
Answer: C. It lies centrally within the cavity, lacks a double decidual sign and contains no yolk sac
A true early intrauterine gestational sac implants ECCENTRICALLY within the endometrium, may show a double decidual sign, and goes on to contain a yolk sac and fetal pole. A pseudogestational sac (seen with some ectopic pregnancies) is a CENTRAL fluid collection within the cavity, lacks the double decidual sign, and contains no yolk sac. Mistaking a pseudosac for an intrauterine pregnancy can falsely reassure and miss a coexisting ectopic — confirm an intrauterine pregnancy only by seeing a yolk sac or fetal pole in an eccentric sac.