Page 5 of 17
RD7.1 | Imaging in Ectopic Pregnancy — SDL Guide (Part 2)
Impact on Diagnosis and Management — Stable vs Unstable, and the Heterotopic Trap
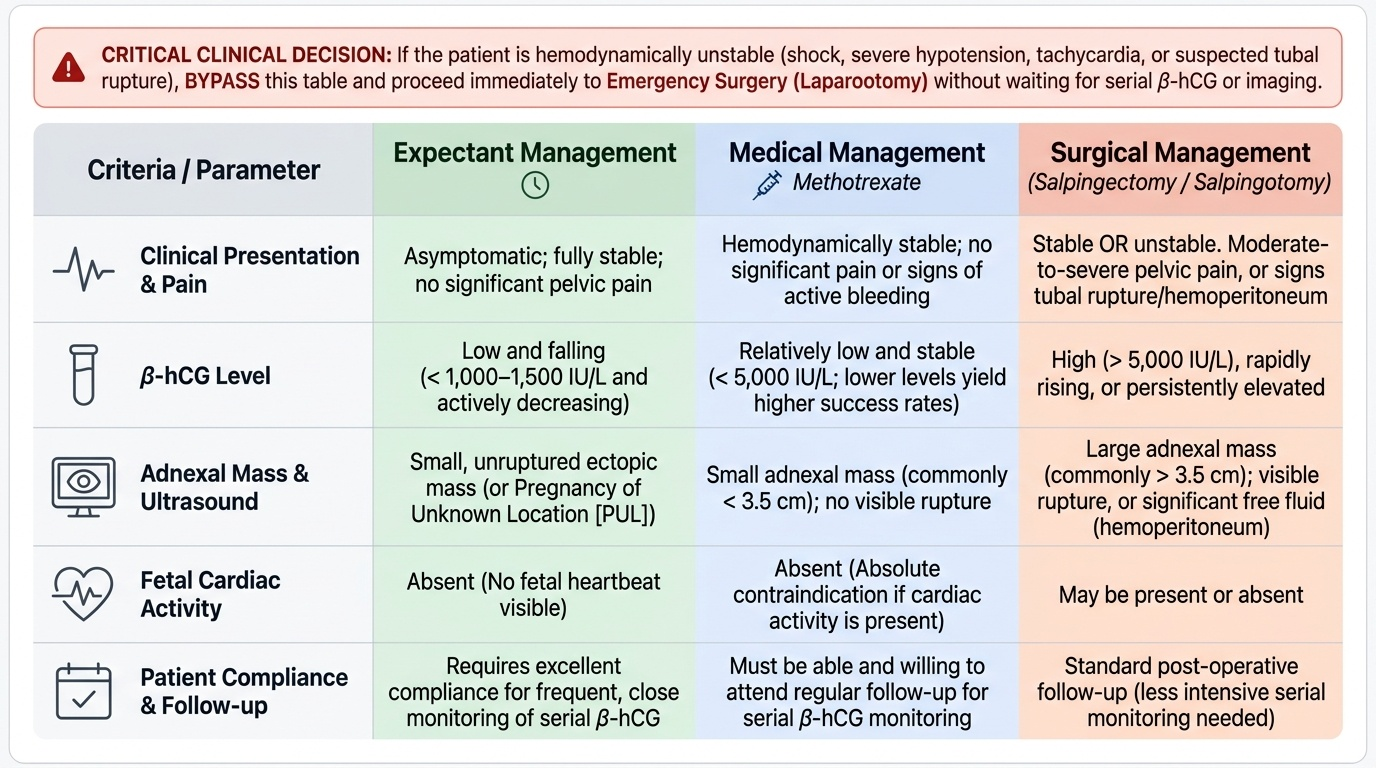
The ultrasound findings and the beta-hCG level translate directly into one of a small number of management pathways, and integrating them correctly is exactly what competency RD7.1 asks of the final-year student. The first and overriding determinant is the patient's haemodynamic state: a woman who is shocked or has signs of rupture is resuscitated and taken for emergency surgery without waiting for the niceties of serial testing. Only in the haemodynamically stable woman does the detailed combination of imaging and hCG select between expectant, medical and surgical management. Throughout, imaging is used to localise and characterise the pregnancy and to monitor the response to non-surgical treatment, while the decision itself rests on the integration of all the findings with the clinical picture.
The unstable patient — surgery first:
Tachycardia, hypotension, peritonism or a large echogenic haemoperitoneum indicate likely tubal rupture. The priority is resuscitation and emergency laparoscopy or laparotomy (usually salpingectomy); imaging must not delay theatre.
The stable patient — imaging and hCG select the route:
- Expectant management may be appropriate for a small, unruptured, asymptomatic ectopic (or a pregnancy of unknown location) with a LOW and FALLING beta-hCG, under close surveillance with serial hCG.
- Medical management with methotrexate suits a stable woman with an unruptured ectopic, no significant pain, no fetal cardiac activity, a relatively low beta-hCG (units commonly use a threshold around 5000 IU/L as a guide, lower is better) and a small adnexal mass, who can attend for follow-up; serial beta-hCG monitors the response.
- Surgical management (laparoscopic salpingectomy or salpingotomy) is indicated for a larger ectopic, significant pain, fetal cardiac activity, a high or rising beta-hCG, or where medical/expectant management has failed or is unsuitable.
Pregnancy of unknown location (PUL):
When TVS shows neither an intrauterine nor an extrauterine pregnancy and the beta-hCG is below the discriminatory zone, the situation is a PUL. This is a temporary classification, not a diagnosis: it is resolved by serial beta-hCG and repeat TVS, watching for a rise that leads to a visible intrauterine pregnancy, a fall consistent with a failing pregnancy, or a plateau/suboptimal rise that points to an ectopic. The cardinal rule is never to discharge a PUL as 'normal'.
The heterotopic trap:
A heterotopic pregnancy — a coexisting intrauterine AND ectopic pregnancy — is rare in spontaneous conception but markedly more common after assisted reproduction (IVF). The danger is complacency: seeing an intrauterine pregnancy does NOT exclude a simultaneous ectopic in the IVF patient with adnexal pain or a mass. Always examine the adnexa even when an intrauterine pregnancy is confirmed, especially after assisted conception.
Provided image
SELF-CHECK
A woman who conceived through IVF presents at 6 weeks with right-sided pelvic pain. Transvaginal ultrasound clearly shows a live intrauterine pregnancy. What is the most important additional step before reassuring her?
A. No further imaging is needed; a confirmed intrauterine pregnancy excludes an ectopic
B. Carefully examine both adnexa, because a heterotopic pregnancy (coexisting intrauterine and ectopic) is markedly more common after IVF
C. Arrange an urgent CT abdomen to look for free fluid
D. Measure beta-hCG only; the level will distinguish a heterotopic pregnancy
Reveal Answer
Answer: B. Carefully examine both adnexa, because a heterotopic pregnancy (coexisting intrauterine and ectopic) is markedly more common after IVF
After assisted reproduction (IVF), heterotopic pregnancy — a coexisting intrauterine and ectopic pregnancy — is far more common than in spontaneous conception. Seeing an intrauterine pregnancy therefore does NOT exclude a simultaneous ectopic in a patient with adnexal pain. The correct step is to examine both adnexa on the same transvaginal scan. Beta-hCG cannot distinguish a heterotopic pregnancy because both gestations contribute to the level, and CT is not the appropriate modality in early pregnancy.
CLINICAL PEARL
Pearl 1 — Read TVS against the beta-hCG, not in isolation. An empty uterus with a beta-hCG ABOVE the discriminatory zone (~1500-2000 IU/L) is an ectopic until proven otherwise; an empty uterus with hCG below the zone is a pregnancy of unknown location requiring serial follow-up — never a reassuring 'normal'.
Pearl 2 — Never assume an intrauterine pregnancy you have not seen, and beware the pseudosac. Confirm an intrauterine pregnancy only by visualising a yolk sac or fetal pole in an eccentric sac. A central cavity fluid collection with no yolk sac and no double decidual sign is a pseudogestational sac and can accompany an ectopic.
Pearl 3 — Examine the adnexa even when you find an intrauterine pregnancy, especially after IVF. Heterotopic pregnancy is rare spontaneously but much commoner after assisted reproduction; an intrauterine pregnancy does not exclude a coexisting ectopic in a woman with adnexal pain or a mass.
Self-Assessment — Imaging-Guided Decisions in Suspected Ectopic
Work through these scenarios as the clinician assessing the patient. For each, decide on the imaging, interpret the findings against the beta-hCG, and reach a management plan before reading the discussion. Integrating imaging and biochemistry into a safe decision is precisely the competence RD7.1 expects.
Scenario A: A 30-year-old woman, 7 weeks by dates, presents with mild left iliac fossa pain and a positive test. She is haemodynamically stable. Beta-hCG is 2500 IU/L. Transvaginal ultrasound shows an empty uterus and a 2 cm adnexal 'tubal ring' separate from the left ovary, with a small amount of free fluid in the pouch of Douglas. What is the diagnosis and what management options should be considered?
Discussion: This is a tubal ectopic pregnancy — the beta-hCG is above the discriminatory zone with an empty uterus, and there is a specific adnexal tubal-ring sign separate from the ovary. As she is stable with a relatively small unruptured ectopic and a low beta-hCG, both medical management with methotrexate (if she has no significant pain, no fetal cardiac activity in the mass, and can attend for follow-up) and laparoscopic surgery are options; the choice depends on local protocol, hCG level, mass size and patient preference. The free fluid warrants careful reassessment for any sign of rupture.
Scenario B: A 24-year-old woman, 5 weeks by dates, has slight spotting and minimal pain. She is stable. Beta-hCG is 800 IU/L. Transvaginal ultrasound shows an empty uterus and no adnexal abnormality. How should this be classified and managed?
Discussion: This is a pregnancy of unknown location (PUL): the beta-hCG is below the discriminatory zone and the scan shows neither an intrauterine nor an extrauterine pregnancy. It must NOT be called normal or discharged as reassured. The correct approach is serial beta-hCG at 48 hours plus repeat transvaginal ultrasound, watching for an appropriate rise leading to a visible intrauterine pregnancy, a fall consistent with a failing pregnancy, or a suboptimal rise/plateau suggesting ectopic. Safety-net advice about pain and bleeding is essential.
Scenario C: A 33-year-old woman collapses at home and arrives with a heart rate of 130, blood pressure 80/50, and a rigid, tender abdomen. Her urine pregnancy test is positive. A focused transabdominal scan shows a large amount of echogenic free fluid in the abdomen and an empty uterus. What is the priority, and what is the role of further imaging?
Discussion: This is a ruptured ectopic pregnancy with haemorrhagic shock. The priority is immediate resuscitation (large-bore access, fluids, blood, crossmatch) and emergency surgery (laparoscopy or laparotomy, usually salpingectomy). Imaging here is confirmatory only — the focused scan showing free fluid and an empty uterus is sufficient — and must NOT delay transfer to theatre. There is no role for waiting on serial beta-hCG or detailed transvaginal assessment in an unstable patient.