Page 7 of 17
RD7.1 | Imaging in Infertility Evaluation — SDL Guide
Learning Objectives
- Frame the female infertility workup in terms of ovarian, tubal and uterine factors and identify where imaging contributes to each.
- Match the appropriate imaging test to the factor being assessed — transvaginal ultrasound for ovarian reserve, ovulation and the uterus; HSG/HyCoSy/laparoscopy for tubal patency; saline infusion sonohysterography for the cavity.
- State the correct timing and contraindications for hysterosalpingography and explain the rationale for the follicular-phase window.
- Describe the expected imaging findings of patent versus blocked tubes, common uterine-cavity lesions, and measures of ovarian reserve.
- Integrate the imaging findings into a fertility management plan, including ovulation induction, tubal surgery versus IVF, and hysteroscopic correction.
INSTRUCTIONS
Infertility — failure to conceive after twelve months of regular unprotected intercourse — affects around one in seven couples and is a common reason for referral. The evaluation is a structured search across three factors in the woman (ovarian, tubal, uterine), alongside the male factor, and imaging is central to it: choosing the right test, performing it at the right time in the cycle, and interpreting it correctly directs the entire fertility plan. As a final-year student you will be expected to understand why a hysterosalpingogram is timed to the follicular phase, when an ultrasound answers the question without radiation, and how a blocked tube or a uterine polyp changes management. This module equips you to integrate these imaging findings into rational, patient-centred care.
References
- Sutton's Textbook of Radiology and Imaging, 7th edition, Chapter on Gynaecological Imaging (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter on the Female Pelvis and Infertility (textbook)
- NICE CG156 — Fertility Problems: Assessment and Treatment (guideline)
- Shaw's Textbook of Gynaecology, Chapter on Infertility (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A couple in their early thirties have been trying to conceive for two years without success. The man's semen analysis is normal. Now attention turns to the woman, and the gynaecologist must build a picture from a small number of well-chosen investigations. Is she ovulating? Are her fallopian tubes open so that egg and sperm can meet? Is the uterine cavity normal so that an embryo could implant? Each of these questions has a different imaging answer, performed at a different time in the cycle and using a different technique — and choosing the wrong test, or the right test at the wrong time, wastes weeks and can even irradiate an early pregnancy. The skill is not in performing the scans but in knowing which test answers which question, and in reading the results into a coherent plan that gives this couple their best chance.
WHY THIS MATTERS
Infertility affects roughly 10-15% of couples, and the female evaluation is one of the most imaging-dependent workups in gynaecology. The NMC competency RD7.1 requires you to integrate provided imaging findings into the evaluation of infertility — a task that demands you understand not just what each test shows but why and when it is chosen. The decisions that follow are consequential and expensive: a tubal block may direct a couple straight to IVF rather than years of futile timed intercourse; a uterine polyp may be a simple, correctable cause; a low ovarian reserve changes the urgency and the counselling. You will encounter subfertile couples in gynaecology, family medicine and increasingly in primary care, and a clear grasp of the imaging strategy — and of radiation safety in women trying to conceive — is directly applicable, examinable, and important to patients.
RECALL
Before reading further, recall:
- Reproductive anatomy (from AN): the egg is released from the ovary, captured by the fimbriae, fertilised in the ampulla of the fallopian tube, and the embryo travels to implant in the endometrial cavity of the uterus. Patency of the tubes and a normal cavity are both prerequisites for natural conception.
- The ovulatory cycle (from PY/OG): in the follicular phase, FSH drives growth of a cohort of antral follicles; one becomes dominant and ovulates at mid-cycle; the luteal phase follows. The number of small antral follicles at the start of the cycle reflects the remaining egg supply, or ovarian reserve.
- Ovarian reserve markers: the antral follicle count (AFC) on transvaginal ultrasound and serum anti-Mullerian hormone (AMH) are the principal markers of ovarian reserve; a low AFC/AMH indicates diminished reserve.
- Radiation safety in women of reproductive potential (RD principle): tests using ionising radiation must be justified and, where possible, replaced by ultrasound; any radiographic test of the pelvis must be performed when the woman cannot be pregnant — for the uterus and tubes this means the follicular phase, after menstruation and before ovulation.
Clinical Scenario — The Subfertile Couple and the Three Questions Imaging Must Answer
The clinical scenario that brings imaging into the infertility workup is the subfertile couple — typically defined as failure to conceive after twelve months of regular unprotected intercourse (or six months if the woman is over 35 or there is a known risk factor). The evaluation is deliberately systematic, because infertility is multifactorial and the couple's time and emotional resources are precious. After confirming a normal semen analysis in the male partner, the female evaluation addresses three structural-functional questions, and imaging contributes to each of them in a specific way. Understanding this framework is what allows you to choose investigations rationally rather than ordering everything at once: each test is selected to answer one of the three questions, at the time in the cycle when it gives a valid answer.
The three questions imaging helps answer are:
- Is she ovulating, and what is her ovarian reserve? Assessed by serial transvaginal ultrasound (follicular tracking) for ovulation and by the antral follicle count for ovarian reserve, alongside hormonal tests (mid-luteal progesterone, AMH).
- Are the fallopian tubes patent? Assessed by hysterosalpingography (HSG), hysterosalpingo-contrast-sonography (HyCoSy), or — definitively — laparoscopy with chromopertubation.
- Is the uterine cavity normal? Assessed by transvaginal ultrasound and, for cavity lesions, saline infusion sonohysterography (SIS); congenital Mullerian anomalies are best characterised by 3D ultrasound or MRI.
Framing the workup as these three questions prevents both omission (forgetting to test the tubes) and redundancy (repeating tests that answer the same question). It also makes radiation stewardship explicit: where an ultrasound-based test answers the question (ovarian reserve, ovulation, cavity, and increasingly tubal patency via HyCoSy), it is preferred over a radiographic test in a woman actively trying to conceive.
Imaging Strategy — Matching the Modality to the Factor Being Tested
The imaging strategy in infertility is best understood as matching each modality to the factor it is designed to assess, because no single test covers all three questions. The guiding principles are familiar from the rest of gynaecological radiology: prefer ultrasound where it answers the question (no ionising radiation, repeatable, well tolerated), reserve radiographic and invasive tests for what only they can show, and time any pelvic radiographic study to the follicular phase to avoid irradiating an early pregnancy. Knowing which test to choose, and when in the cycle to perform it, is the practical core of competency RD7.1 in this setting. Each test below is selected for a specific factor and has its own timing and safety considerations.
Ovarian reserve and ovulation — transvaginal ultrasound (TVS):
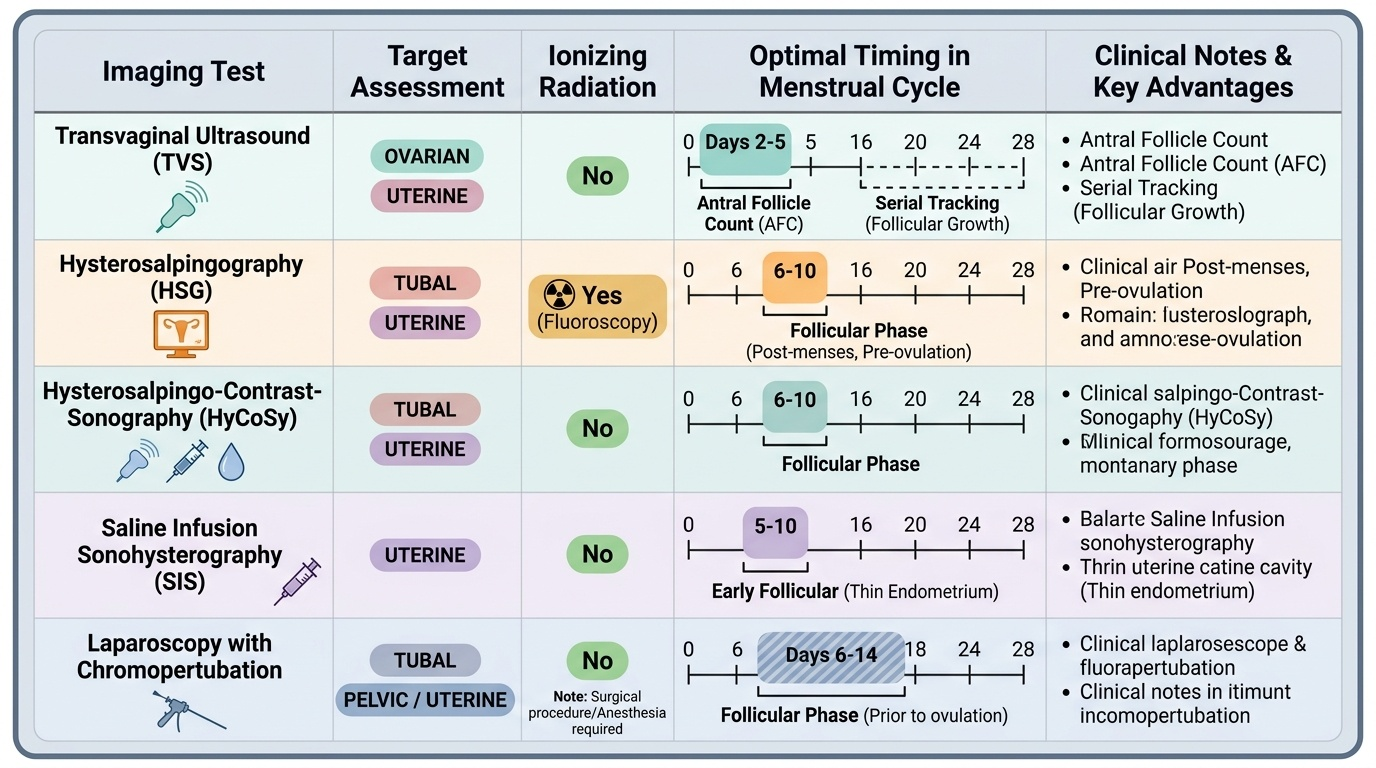
The antral follicle count (AFC), the number of small 2-10 mm follicles across both ovaries, is measured by TVS in the early follicular phase and reflects ovarian reserve. Follicular tracking is serial TVS through the cycle to confirm growth of a dominant follicle and ovulation, used both diagnostically and during ovulation-induction treatment.
Tubal patency — HSG, HyCoSy or laparoscopy:
- Hysterosalpingography (HSG) is a fluoroscopic test in which iodinated contrast is instilled through the cervix to outline the uterine cavity and fallopian tubes; free peritoneal spill confirms patency. It is the conventional standard for tubal assessment. It must be performed in the follicular phase, classically days 6-10 of the cycle — after menstruation has stopped (so the cavity is not obscured by blood or clot) and before ovulation (so an early pregnancy is not irradiated). It is contraindicated in pregnancy and in active pelvic infection, and active or recent pelvic inflammatory disease must be excluded first.
- Hysterosalpingo-contrast-sonography (HyCoSy) is the ultrasound-based, radiation-free alternative, instilling an ultrasound contrast/saline-air medium and watching tubal flow on TVS; it correlates well with HSG and avoids both ionising radiation and iodinated contrast.
- Laparoscopy with chromopertubation (instilling methylene-blue dye and observing spill from the fimbrial ends) is the definitive, gold-standard test of tubal patency and also visualises pelvic pathology such as endometriosis and adhesions; it is reserved for when less invasive tests are inconclusive or pelvic pathology is suspected.
Uterine cavity and anomalies — SIS and MRI/3D-USG:
- Saline infusion sonohysterography (SIS) distends the cavity with sterile saline during TVS to delineate endometrial polyps, submucous fibroids, intrauterine adhesions and a septum — lesions that may impair implantation.
- 3D ultrasound or MRI best characterises congenital Mullerian anomalies (e.g. septate, bicornuate, unicornuate uterus), which MRI distinguishes by the external fundal contour, an important distinction because management differs.
Throughout, CT has essentially no role in routine infertility imaging — it delivers ionising radiation with no advantage for assessing the uterus, tubes or ovaries.
Provided image
SELF-CHECK
A gynaecologist plans a hysterosalpingogram (HSG) to assess tubal patency in a woman being investigated for infertility. What is the correct timing in the menstrual cycle, and what is the principal reason for it?
A. Just before menstruation, so that the endometrium is thickest and most clearly outlined
B. The follicular phase, classically days 6-10 — after menstruation has stopped and before ovulation, to avoid irradiating an early pregnancy and to image a clear, non-bleeding cavity
C. At mid-cycle ovulation, to confirm the dominant follicle at the same time
D. Any time in the cycle, as timing does not affect an HSG
Reveal Answer
Answer: B. The follicular phase, classically days 6-10 — after menstruation has stopped and before ovulation, to avoid irradiating an early pregnancy and to image a clear, non-bleeding cavity
HSG uses ionising radiation and iodinated contrast, so it is performed in the follicular phase (classically days 6-10) — after menstruation has finished, so blood and clot do not obscure the cavity, and before ovulation, so an early pregnancy is not inadvertently irradiated. Pregnancy and active pelvic infection must be excluded first. Performing it in the luteal phase risks irradiating an early conception; mid-cycle is not the indication.
Expected Imaging Findings — Patent vs Blocked Tubes, Cavity Lesions and Ovarian Reserve
Interpreting the findings of the infertility imaging tests is what converts a list of investigations into a diagnosis, and each test has a characteristic normal and abnormal appearance you must be able to recognise. The unifying theme is that the findings map directly onto the three questions: tubal tests show whether contrast or dye reaches the peritoneal cavity, cavity tests show whether the endometrial cavity is smooth and unobstructed, and ovarian assessment counts the follicles that represent egg supply. Because these findings drive very different management routes — from simple ovulation induction to IVF — accurate interpretation, read in the context of the whole workup, is essential. The descriptions below are the appearances you are most likely to be shown and asked to integrate.
Tubal patency (HSG / HyCoSy):
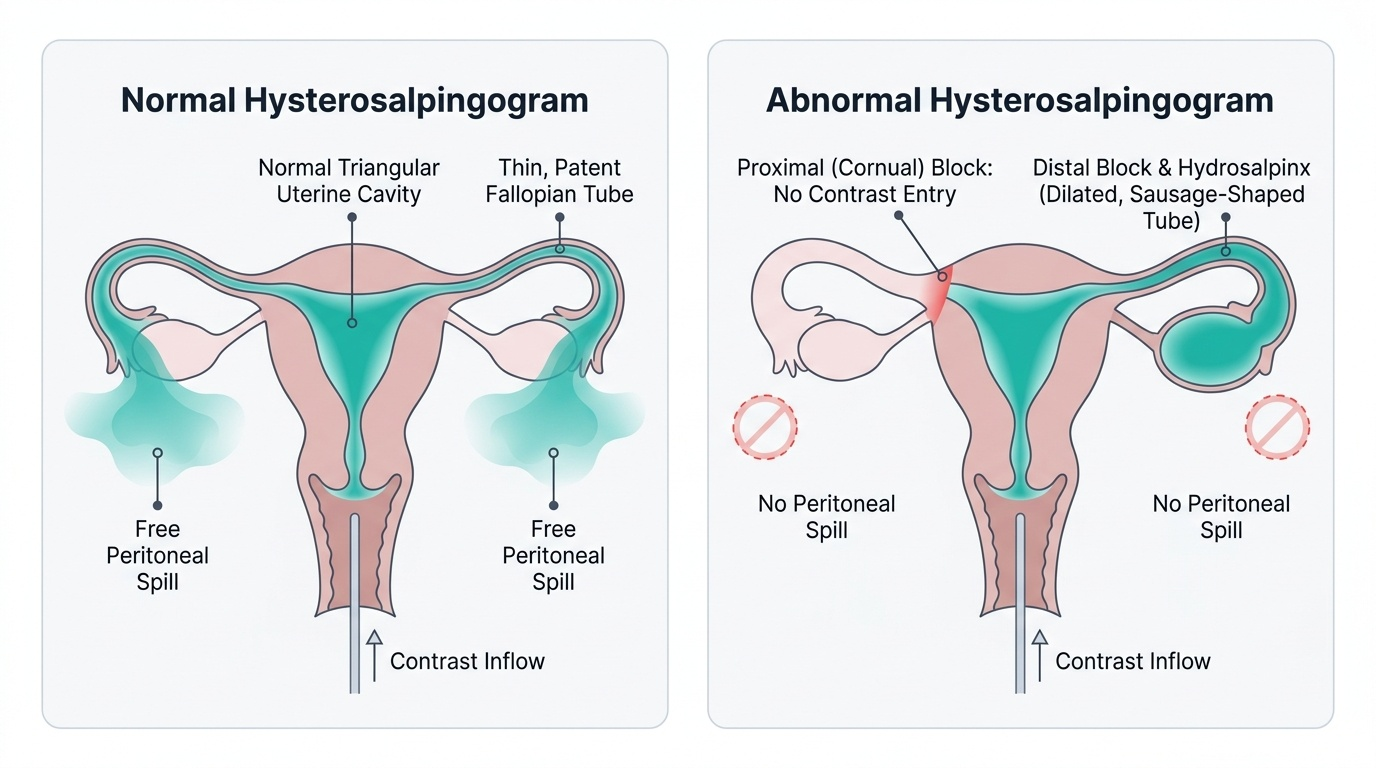
- Normal/patent: contrast (or ultrasound medium) fills a normal triangular uterine cavity, passes along thin tubular fallopian tubes, and shows free peritoneal spill at the fimbrial ends bilaterally — the hallmark of patent tubes.
- Tubal block: contrast fails to pass beyond a point in the tube with no peritoneal spill. A proximal (cornual) block may be genuine or a false positive from cornual spasm (a recognised pitfall — repeat or laparoscopy may be needed to confirm). A distal block with a fluid-distended tube produces a hydrosalpinx, a sausage-shaped dilated tube that retains contrast and is associated with poor fertility outcomes.
Uterine cavity (TVS / SIS):
- Endometrial polyp: a focal echogenic intracavitary lesion outlined by saline on SIS.
- Submucous fibroid: a hypoechoic mass indenting or filling the cavity.
- Intrauterine adhesions (Asherman): bridging bands or an irregular, partly obliterated cavity.
- Septum: a tissue partition dividing the cavity, best characterised (against bicornuate uterus) by the external fundal contour on 3D ultrasound or MRI.
Ovarian reserve and ovulation (TVS):
- Antral follicle count (AFC): a count of small 2-10 mm follicles across both ovaries; a low AFC indicates diminished ovarian reserve, while a high count may reflect polycystic ovarian morphology (linking to the PCOD assessment).
- Follicular tracking: serial scans showing a follicle growing to ~18-24 mm and then collapsing with appearance of luteal changes confirms ovulation.
Provided image
SELF-CHECK
A hysterosalpingogram shows contrast filling a normal uterine cavity and passing into the right tube with free peritoneal spill, but on the left the contrast stops at the cornu with no flow into the tube. The patient experienced cramping during the procedure. What is the most appropriate interpretation?
A. Definite bilateral tubal block requiring immediate IVF
B. The right tube is patent; the apparent left proximal (cornual) block may be genuine OR a false positive from cornual spasm, so it should be confirmed (e.g. repeat study or laparoscopy with dye)
C. Normal study — unilateral spill confirms both tubes are patent
D. Hydrosalpinx of the left tube, which is diagnostic of distal block
Reveal Answer
Answer: B. The right tube is patent; the apparent left proximal (cornual) block may be genuine OR a false positive from cornual spasm, so it should be confirmed (e.g. repeat study or laparoscopy with dye)
Free peritoneal spill on the right confirms a patent right tube. An apparent proximal (cornual) block, especially with cramping, is a recognised pitfall because cornual spasm can mimic genuine occlusion (a false positive). It should therefore be confirmed before acting — by repeating the study, using antispasmodics, or proceeding to laparoscopy with chromopertubation (the gold standard). A hydrosalpinx is a dilated, fluid-filled tube indicating DISTAL block, not the cornual appearance described here.