Page 8 of 17
RD7.1 | Imaging in Infertility Evaluation — SDL Guide (Part 2)
Impact on Diagnosis and Management — From Findings to a Fertility Plan
The purpose of the entire imaging workup is to build a fertility plan, and the integration of the findings into management is exactly what competency RD7.1 expects of the final-year student: take the provided imaging findings across the three factors and translate them into the next step for the couple. Management is rarely driven by one test in isolation; rather, the picture as a whole — ovulatory status and reserve, tubal patency, and cavity normality, together with the male factor and the woman's age — determines whether the couple is offered simple measures, a corrective procedure, or assisted reproduction. The discipline is to read each finding for its management implication and to weigh the findings together rather than reflexively escalating on a single abnormality.
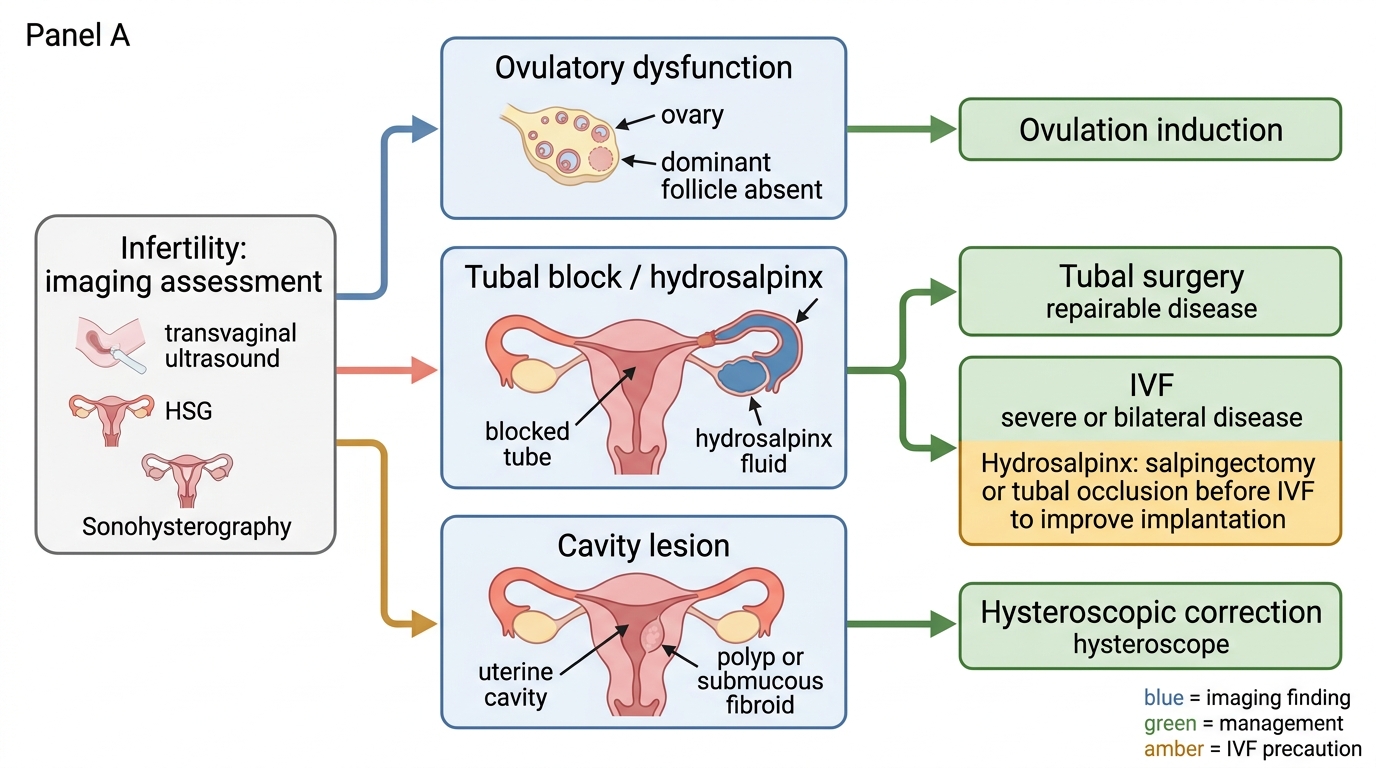
Ovulatory dysfunction or anovulation (from follicular tracking / hormonal tests):
- The cornerstone is ovulation induction (e.g. letrozole as first-line, or clomifene), with follicular-tracking ultrasound monitoring follicle growth and timing intercourse, insemination or trigger. Here imaging is an active treatment-monitoring tool, not just a diagnostic one.
- A diminished ovarian reserve (low AFC/AMH) adds urgency to counselling and may move the couple sooner towards IVF.
Tubal block (from HSG / HyCoSy / laparoscopy):
- A proximal block may be amenable to tubal cannulation or surgery if genuine, but cornual spasm must first be excluded.
- A hydrosalpinx (distal block) reduces IVF success and is often best treated by salpingectomy or tubal occlusion before IVF, because the fluid is toxic to implantation.
- Bilateral tubal block generally directs the couple to IVF, which bypasses the tubes altogether, rather than years of unsuccessful natural attempts.
Uterine-cavity lesion (from SIS / hysteroscopy):
- An endometrial polyp, submucous fibroid or intrauterine adhesion that distorts the cavity is typically corrected by hysteroscopic removal/resection to improve implantation.
- A uterine septum may be resected hysteroscopically in selected cases; distinguishing it from a bicornuate uterus (by fundal contour on MRI/3D-USG) is essential because the latter is managed differently.
The overarching message is that imaging in infertility is not a box-ticking exercise but a directed search whose findings change the path the couple takes — from a tablet and a tracking scan, to a hysteroscopic day-case, to IVF. Reading the imaging into that decision, with attention to radiation safety and timing, is the applied competence this module builds.
Infertility Imaging Findings and Management
SELF-CHECK
A 34-year-old woman with infertility is found on HSG to have a left hydrosalpinx (dilated, fluid-filled, distally blocked tube) and a blocked right tube. Her ovarian reserve is adequate and the cavity is normal. The couple are counselled towards IVF. What additional management does the hydrosalpinx specifically warrant before IVF, and why?
A. No specific action; the hydrosalpinx does not affect IVF outcomes
B. Salpingectomy or tubal occlusion of the hydrosalpinx before IVF, because the retained fluid reduces implantation and lowers IVF success
C. Repeated HSG every month to monitor the hydrosalpinx
D. Immediate methotrexate to shrink the hydrosalpinx
Reveal Answer
Answer: B. Salpingectomy or tubal occlusion of the hydrosalpinx before IVF, because the retained fluid reduces implantation and lowers IVF success
A hydrosalpinx is a distally blocked, fluid-filled tube. The retained fluid can reflux into the uterine cavity and is toxic to the endometrium and embryo, significantly reducing IVF implantation and success rates. Current practice is therefore to remove (salpingectomy) or occlude the affected tube before IVF. With bilateral tubal disease, IVF (which bypasses the tubes) is the appropriate route, but the hydrosalpinx should be dealt with first. Methotrexate has no role here.
CLINICAL PEARL
Pearl 1 — Match the test to the factor. Transvaginal ultrasound assesses ovarian reserve (antral follicle count), ovulation (follicular tracking) and the uterus/cavity; HSG, HyCoSy or laparoscopy assess tubal patency; SIS assesses cavity lesions. Asking 'which of the three questions am I answering?' chooses the test.
Pearl 2 — Time the HSG to the follicular phase (days 6-10) and exclude pregnancy and infection first. This avoids irradiating an early pregnancy, images a clean non-bleeding cavity, and prevents flaring active pelvic infection. Where radiation can be avoided, HyCoSy answers the same tubal question without ionising radiation.
Pearl 3 — Beware the false-positive cornual block, and treat a hydrosalpinx before IVF. An apparent proximal block on HSG may be cornual spasm — confirm with laparoscopy/dye before acting. A hydrosalpinx lowers IVF success, so salpingectomy or occlusion is advised before proceeding to IVF.
Self-Assessment — Choosing and Interpreting Imaging in the Infertility Workup
Work through these scenarios as the clinician planning the couple's investigations. For each, decide which imaging test answers the question, when it should be done, and how the result would change management, before reading the discussion. Integrating the right test, performed at the right time, into a management plan is the applied competence RD7.1 sets for you.
Scenario A: A couple have failed to conceive for 18 months. The man's semen analysis is normal. The woman has regular cycles. The gynaecologist wants to confirm tubal patency. She is keen to avoid radiation if possible. What test would you offer, and when in the cycle?
Discussion: Tubal patency is the question. The radiation-free option is HyCoSy (hysterosalpingo-contrast-sonography), which assesses tubal flow on ultrasound and avoids both ionising radiation and iodinated contrast; conventional HSG is the alternative. Either is performed in the follicular phase (classically days 6-10), after menstruation has stopped and before ovulation, with pregnancy and active pelvic infection excluded first. If the result is inconclusive (e.g. a possible cornual block from spasm), laparoscopy with chromopertubation is the definitive confirmatory test.
Scenario B: A woman with secondary infertility had a previous dilatation and curettage after a miscarriage and now has very light periods. Transvaginal ultrasound suggests an irregular endometrium. Which test best assesses the cavity, and what are you looking for?
Discussion: The history (instrumentation, light periods, secondary infertility) raises suspicion of intrauterine adhesions (Asherman syndrome). Saline infusion sonohysterography (SIS) distends the cavity to reveal bridging adhesions or an irregular, partly obliterated cavity; hysteroscopy both confirms and treats them. Correcting the adhesions hysteroscopically can restore cavity normality and improve fertility.
Scenario C: A 29-year-old woman with infertility has a transvaginal ultrasound showing a low antral follicle count and an HSG showing bilateral tubal patency with free spill. She is ovulating on follicular tracking. How do you read this combination and what does it imply for management?
Discussion: The tubes are patent and she is ovulating, so the tubal and ovulatory mechanics are favourable — but the low antral follicle count indicates diminished ovarian reserve, which is the key finding here. This adds urgency to counselling and may move the couple towards earlier assisted reproduction, alongside confirming the male factor and lifestyle optimisation. The imaging integrates into a plan that prioritises time, given the reserve.