Page 1 of 8
RD6.1 | Procedure-specific Written and Verbal Patient Instructions — SDL Guide
Learning Objectives
- Explain why correct, procedure-specific patient preparation is a clinician responsibility at the point of referral, not only a radiology-department task.
- State the governing principles behind fasting, full-bladder, bowel, hydration, contrast-safety and MRI device-safety preparation.
- Write and deliver matched written AND verbal instructions tailored to the patient and the imaging procedure (USG, barium studies, IVU/contrast-enhanced CT, MRI).
- Verify before the procedure that preparation succeeded and that contrast and MRI safety screening results are within safe thresholds, recognising the red flags that mandate deferral.
- Tailor instructions for special situations: the diabetic on metformin, the pregnant patient, the patient with renal impairment, and the patient with a possible ferromagnetic implant or foreign body.
INSTRUCTIONS
An imaging request is only as good as the preparation that precedes it. A gallbladder ultrasound on a patient who has just eaten, a contrast CT in a patient whose renal function was never checked, or an MRI on a patient with an unscreened cardiac device are all preventable failures — and every one of them begins at the moment the clinician orders the scan and counsels the patient. This module builds the practical skill described in NMC competency RD6.1: the ability to provide written and verbal instructions tailored to the patient and the imaging procedure, including fasting requirements, medication adjustments and bowel preparation. You will learn the reasoning behind each instruction, the exact procedure-specific content to communicate, and how to confirm that preparation was done before the patient enters the scanner.
References
- Sutton's Textbook of Radiology and Imaging, 8th edition (Patient Preparation and Contrast Media) (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter on Contrast Media and Patient Safety (textbook)
- European Society of Urogenital Radiology (ESUR) Guidelines on Contrast Media, v10 (guideline)
- Atomic Energy Regulatory Board (AERB) Safety Code for Medical Diagnostic Radiology, India (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 8 a.m. in the outpatient department. A 52-year-old woman with right-upper-quadrant pain returns for her abdominal ultrasound, which you arranged last week to look for gallstones. The sonographer calls you: her gallbladder is collapsed and uninterpretable because she ate a full breakfast on the way in — nobody told her to fast. The slot is lost, she must return another day, and her diagnosis is delayed. Down the corridor, a 60-year-old man on metformin is about to have a contrast-enhanced CT; his request form has no recorded kidney function, and the radiographer is asking whether it is safe to inject. Two scans, two patients, and the same root cause: preparation instructions that were either never given or never confirmed. Neither failure is a radiology-department problem — both started with the clinician who ordered the scan.
WHY THIS MATTERS
Patient preparation is one of the highest-yield, lowest-cost clinical skills you will use every week as a primary-care and ward doctor, yet it is rarely taught explicitly. The NMC competency RD6.1 places the responsibility squarely on the requesting clinician: you must be able to provide written and verbal instructions tailored to the individual patient and the specific imaging procedure — fasting requirements, medication adjustments such as withholding metformin, and bowel preparation. Getting this right prevents a cascade of harms: a wasted appointment and a delayed diagnosis when a gallbladder scan is non-diagnostic; an avoidable second dose of ionising radiation when a contrast study must be repeated; contrast-associated kidney injury when renal function was never checked; and, in the MRI suite, a genuine danger to life when a ferromagnetic implant goes unscreened. This skill is examined in clinical postings, OSCE/OSPE stations and professional examinations, and — far more importantly — it is exercised in every real imaging referral you will ever make.
RECALL
Before reading further, recall the modality principles you learned in the foundation SDL of this course:
- Ionising vs non-ionising modalities: X-ray, fluoroscopy, CT and nuclear medicine use ionising radiation; ultrasound (USG) and MRI do not. This is why pregnancy must be excluded before ionising studies but is not a radiation issue for USG/MRI.
- Iodinated contrast (used in CT, IVU and fluoroscopy) is excreted by the kidneys and can precipitate contrast-associated acute kidney injury (CA-AKI), especially when the estimated glomerular filtration rate (eGFR) is low; it also interacts with metformin.
- Gadolinium contrast (used in MRI) carries a risk of nephrogenic systemic fibrosis (NSF) in severe renal failure.
- The MRI magnet is always on: the strong static magnetic field attracts ferromagnetic objects and can heat or displace certain implants — which is why device and foreign-body screening is mandatory.
- Ultrasound depends on an acoustic window: a fasting, distended gallbladder or a full urinary bladder gives the sound waves a clear path, which is why these preparations improve image quality.
If any of these feel hazy, a quick review of the modalities-and-contrast SDL before continuing will make the instructions below much easier to reason about rather than memorise.
Why Correct Patient Preparation Is a Primary-Care Skill
Patient preparation sits at the interface between the clinician's request and the radiology department's execution, and it is precisely at this interface that most preventable imaging failures occur. When a clinician orders a scan, the imaging examination has not yet been made possible — it has only been requested. The diagnostic value of that scan is created in the hours before the patient arrives, by instructions that the patient must understand and act on correctly. An ultrasound of the gallbladder performed on a non-fasted patient is technically a completed scan but a clinically wasted one; a contrast study ordered without a documented kidney function is a safety incident waiting to happen. The clinician who orders an investigation therefore owns the preparation, because only the ordering clinician knows the clinical question, the patient's comorbidities, their medications, and their ability to follow instructions. Treating preparation as 'something the radiology department sorts out' is the single most common reason scans are repeated, delayed, or rendered uninterpretable.
The competency RD6.1 makes two demands that are easy to under-deliver. First, instructions must be procedure-specific — the preparation for an abdominal ultrasound is different from a pelvic ultrasound, which differs again from a barium enema or a contrast CT. Second, instructions must be delivered in both written and verbal form, because each channel covers the other's weakness: verbal counselling lets you check understanding and answer questions in the patient's own language, while a written sheet survives the journey home and carries the date, time, location and a contact number. The harms of getting this wrong are concrete and recurrent:
- Wasted appointment and delayed diagnosis — a non-fasted gallbladder scan or an empty-bladder pelvic scan must be rebooked.
- Avoidable repeat radiation — a non-diagnostic CT or barium study repeated because of inadequate bowel preparation doubles the dose.
- Preventable contrast harm — CA-AKI or metformin-related risk when renal function and medication were not reviewed before iodinated contrast.
- Direct physical danger — a ferromagnetic object or unscreened implant entering the MRI room.
Provided image
Governing Principles — Fasting, Hydration, Contrast and Device Safety
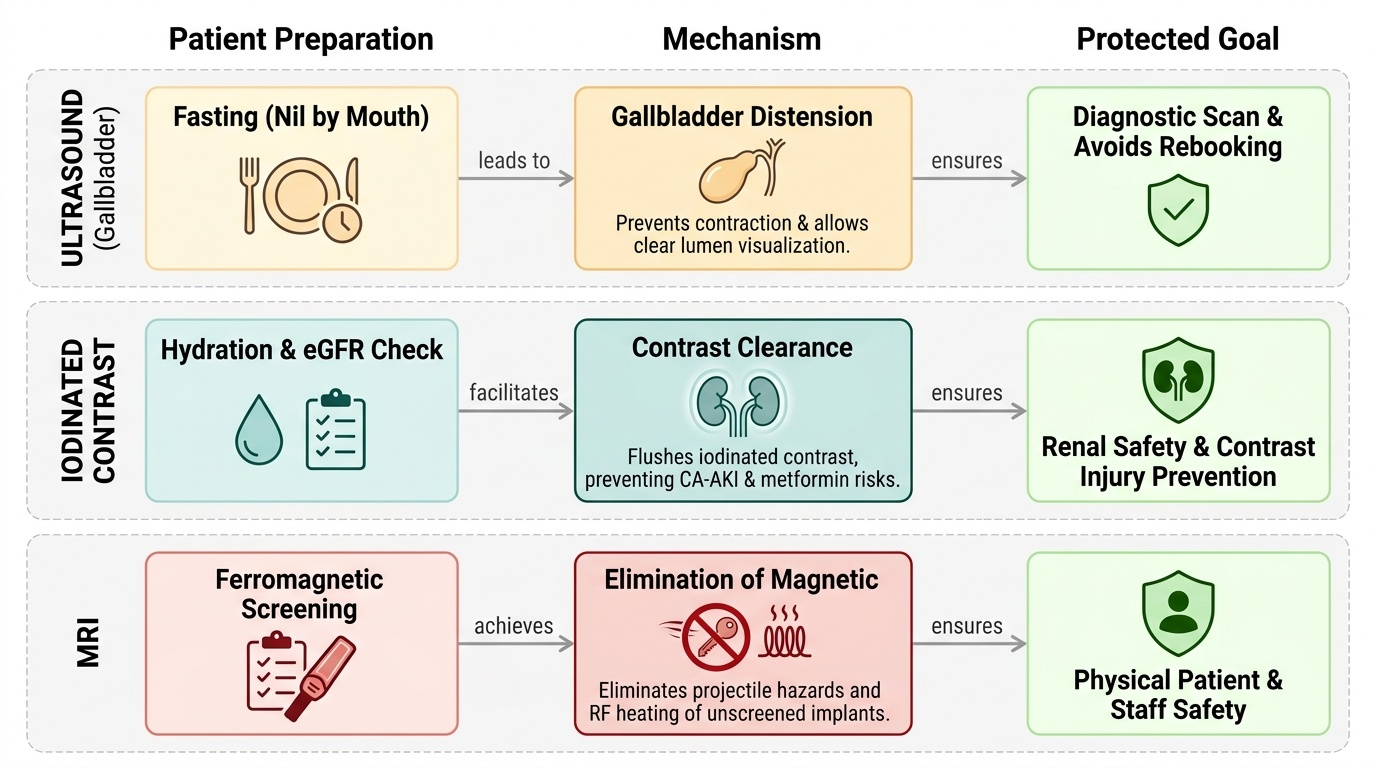
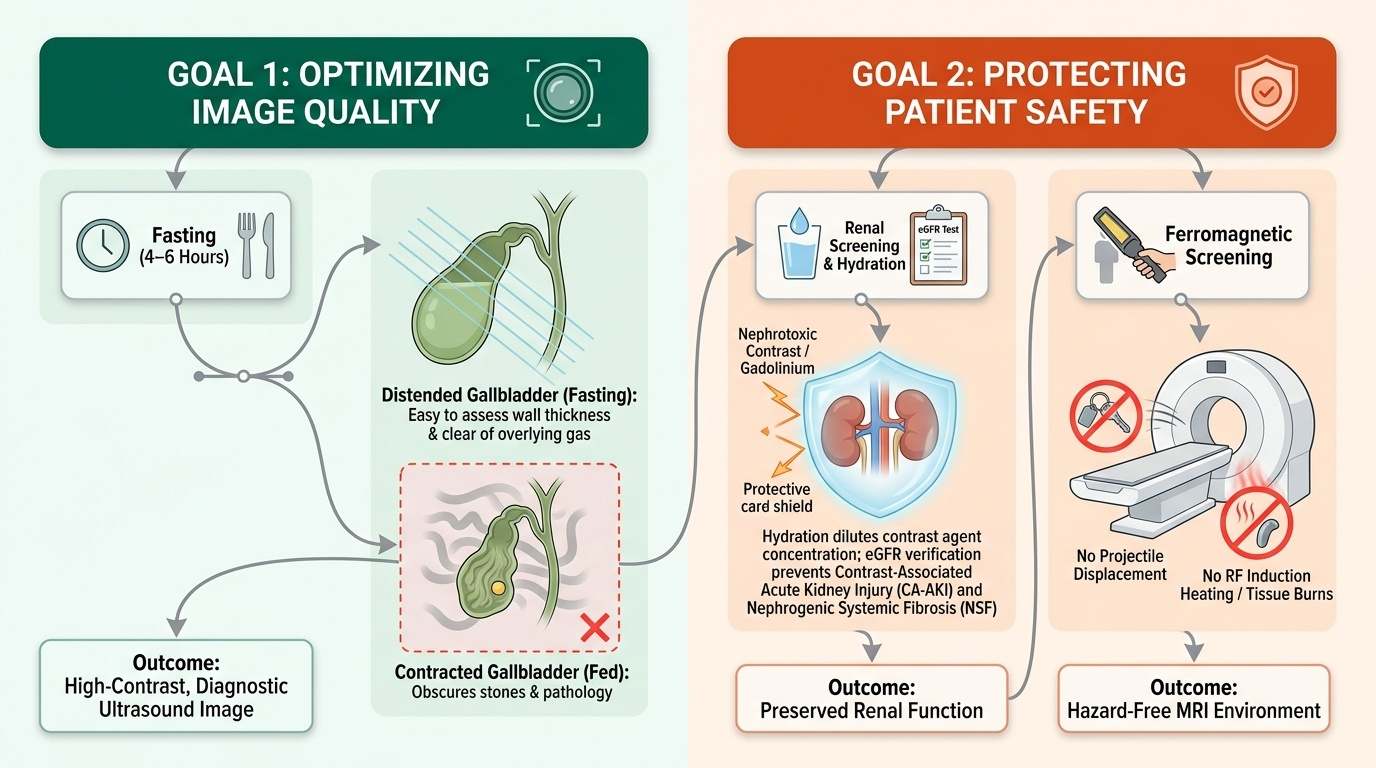
Every preparation instruction exists to protect one of two things: the quality of the image or the safety of the patient. Understanding which goal a given instruction serves turns a long list to be memorised into a short set of principles to be reasoned from, and lets you adapt correctly when a patient's circumstances do not match the standard sheet. Image-quality preparations manipulate the patient's internal state so the modality can see what it needs to: fasting and bladder-filling for ultrasound, and bowel preparation for barium studies. Safety preparations protect the patient from the hazards specific to a modality: renal protection and allergy/medication review for iodinated contrast, renal screening for gadolinium, and ferromagnetic screening for the MRI environment. A clinician who can name the goal behind each instruction can explain it convincingly to a patient — and patients who understand why a step matters are far more likely to comply.
The principles, grouped by goal, are:
- Fasting for abdominal ultrasound (image quality): a 4–6 hour fast empties the stomach and duodenum (reducing overlying gas) and, crucially, allows the gallbladder to distend with bile rather than contract after a meal. A contracted gallbladder hides small stones and cannot be assessed for wall thickening.
- Full bladder for pelvic and obstetric ultrasound (image quality): a distended bladder displaces gas-filled bowel out of the pelvis and provides an acoustic window to the uterus, adnexa and early pregnancy. The patient drinks water and does not void before the scan (transabdominal technique).
- Bowel preparation for barium studies (image quality): residual faeces mimic or obscure mucosal lesions, so a barium enema requires a low-residue diet and bowel cleansing (laxative ± cleansing enema); barium swallow/meal needs only fasting.
- Hydration, renal function, metformin and allergy review for iodinated contrast (safety): iodinated contrast is nephrotoxic in vulnerable kidneys, so eGFR is checked; good hydration reduces CA-AKI risk; metformin is reviewed because it can accumulate if the kidneys are injured by contrast; and a prior contrast reaction history guides premedication or an alternative.
- Renal screening for gadolinium (safety): gadolinium can cause nephrogenic systemic fibrosis in severe renal failure, so eGFR is checked before MRI contrast.
- Ferromagnetic and implant screening for MRI (safety): because the magnet is always on, every patient is screened for cardiac devices, cochlear implants, aneurysm clips and intra-ocular metal, and asked to remove all removable metal objects.
Finally, two communication principles govern HOW instructions are given. Instructions must be legible and language-appropriate — written in a language the patient reads, with simple words, the date, time, location and a contact number — and they must be confirmed by teach-back, where the patient repeats the key steps in their own words so you can detect a misunderstanding before it wastes a scan.
Provided image
Method — Writing and Delivering Procedure-specific Instructions
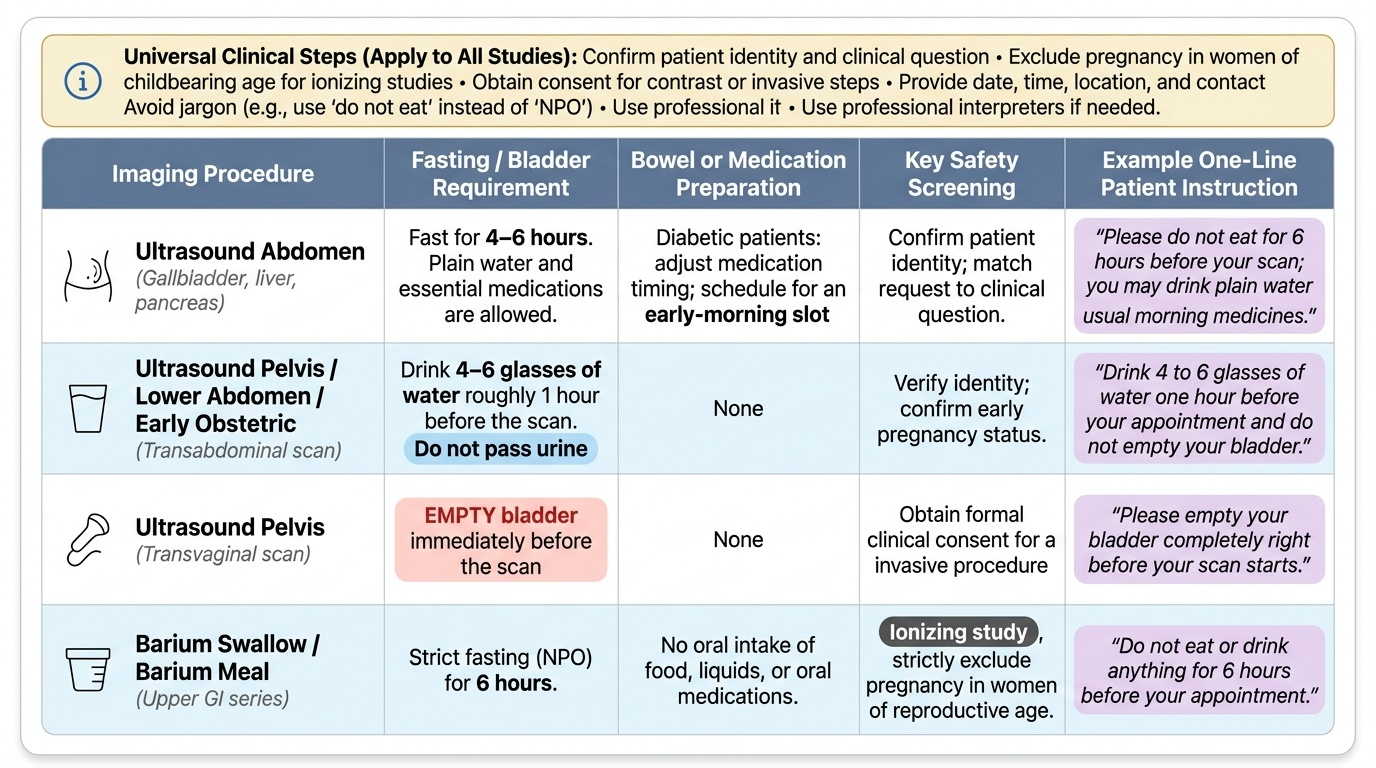
With the principles in place, the practical task is to translate them into clear, procedure-specific instructions and to deliver them in matched written and verbal form. The method is the same for every procedure: identify the exact preparation the modality and the clinical question demand, write it as a short numbered list the patient can follow at home, and then counsel the patient verbally, finishing with a teach-back check. Always include the generic elements that apply to every study — confirm the patient's identity and that the request matches the clinical question, obtain consent where contrast or an invasive step is involved, exclude pregnancy before any ionising study in a woman of reproductive age, and give the date, time, location and a contact number for queries. Never assume literacy or fluency: read the sheet aloud if needed, use an interpreter rather than a relative for critical safety questions, and avoid jargon (say 'do not eat for six hours', not 'remain nil per oral').
The procedure-specific content, delivered in both channels, is:
- Ultrasound abdomen (gallbladder/biliary, liver, pancreas): fast for 4–6 hours (water and essential medicines allowed); diabetic patients should be advised on timing of medication and an early-morning slot.
- Ultrasound pelvis / lower abdomen / early (first-trimester) obstetric (transabdominal): drink about 4–6 glasses of water roughly an hour before and do not pass urine so the bladder is full. (Transvaginal scans need an EMPTY bladder — tell the patient which technique applies.)
- Barium swallow / barium meal (upper GI): fast for about 6 hours; no bowel cleansing needed; warn that stools will be chalky-white for a day or two and that good hydration prevents constipation.
- Barium enema (lower GI): low-residue diet for 1–2 days, a prescribed laxative the evening before, and a cleansing enema as instructed; fast on the morning of the study.
- IVU and contrast-enhanced CT (iodinated contrast): confirm and record a recent eGFR; ensure good oral hydration; review metformin and instruct the patient per protocol; ask about prior contrast reactions and allergies; a light fast (about 4 hours) is commonly advised to reduce nausea, while encouraging clear fluids for hydration.
- MRI (with or without gadolinium): complete the MRI safety questionnaire; remove all metal (jewellery, watches, hairpins, hearing aids, removable dental plates, coins, cards); declare cardiac pacemakers/ICDs, cochlear implants, aneurysm clips and any history of metal in the eyes (an orbital X-ray may be needed first); if gadolinium is planned, confirm eGFR. No routine fasting is needed unless sedation or a specific protocol requires it.
Provided image
SELF-CHECK
You are arranging an abdominal ultrasound to look for gallstones in a 45-year-old woman. What is the single most important preparation instruction you must give, and why?
A. Drink 4–6 glasses of water and do not pass urine, to fill the bladder
B. Fast for 4–6 hours, so the gallbladder distends with bile and can be assessed
C. Take a laxative the night before, to clear the bowel
D. Stop metformin for 48 hours before the scan
Reveal Answer
Answer: B. Fast for 4–6 hours, so the gallbladder distends with bile and can be assessed
For an abdominal (gallbladder/biliary) ultrasound the key preparation is a 4–6 hour fast. Eating triggers gallbladder contraction; a contracted gallbladder can hide small stones and cannot be assessed for wall thickness. The full-bladder instruction is for PELVIC/obstetric transabdominal scans, not the gallbladder. Bowel preparation is for barium enema, and metformin withholding relates to iodinated contrast — neither is relevant to a plain ultrasound, which uses no ionising radiation and no contrast.