Page 2 of 8
RD6.1 | Procedure-specific Written and Verbal Patient Instructions — SDL Guide (Part 2)
Confirming Preparation Was Done — Pre-procedure Checks and Red Flags
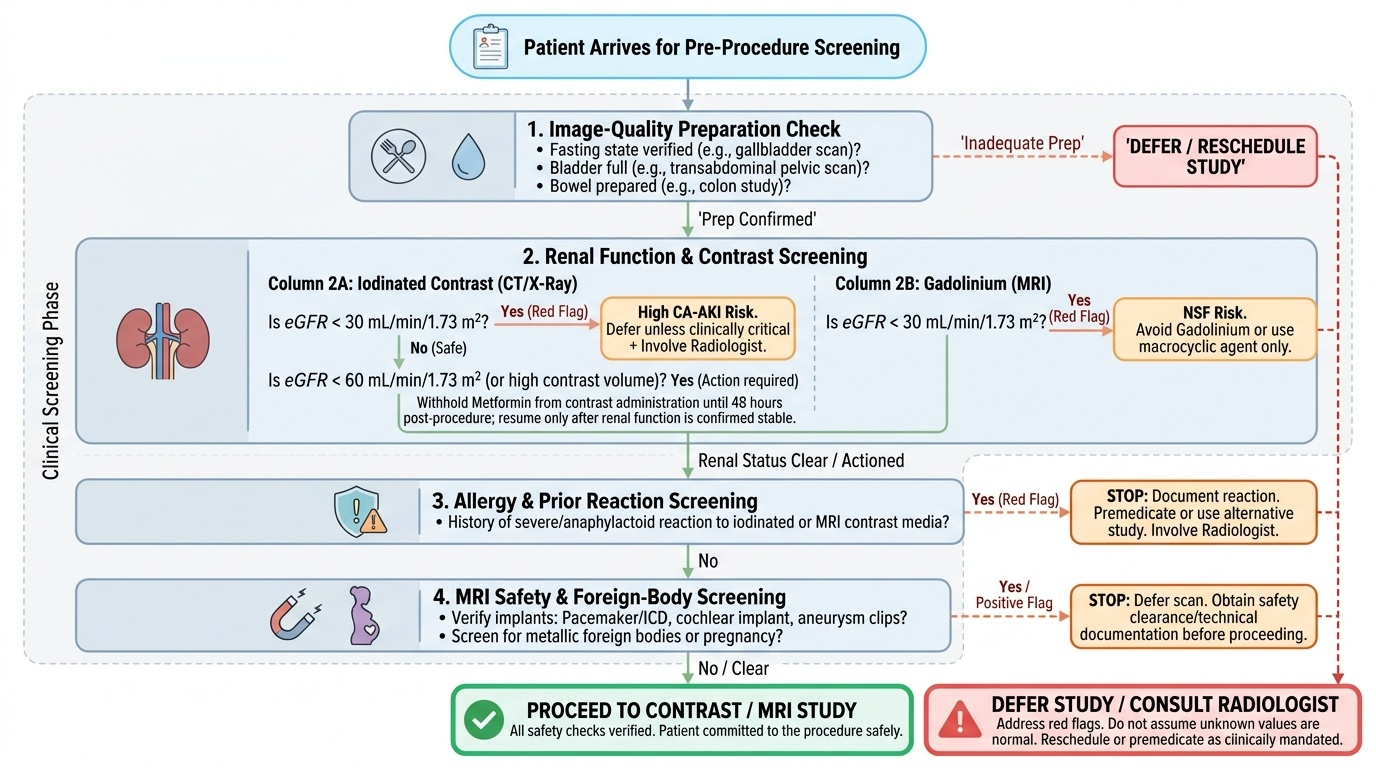
Giving instructions is only half the skill; the other half is verifying, at the door, that preparation actually succeeded and that the safety screening results are within safe limits before the patient is committed to the procedure. This final check is where good instruction prevents harm, because it is the last point at which an unsafe study can be deferred. The check has two parts: confirming the image-quality preparation (did the patient fast? is the bladder full? was the bowel prepared?) and reviewing the safety screening data against defined thresholds (what is the eGFR? was metformin handled? any allergy? is implant and pregnancy screening clear?). Crucially, you are not looking for reassurance — you are actively hunting for the red flag that means STOP. A documented value you cannot see is the same as a value that does not exist: if the eGFR is not on the form, treat it as unknown and obtain it before injecting contrast rather than assuming it is normal.
The pre-procedure verification, with the thresholds and red flags that mandate caution or deferral, is:
- Fasting / bladder / bowel state: confirm verbally and reschedule rather than scan a non-fasted gallbladder, an empty bladder for a transabdominal pelvic scan, or an inadequately prepared colon.
- Renal function for iodinated contrast: review the eGFR. Heightened risk of contrast-associated AKI appears at eGFR <30 mL/min/1.73 m²; below this, intravenous iodinated contrast is given only when no alternative answers the clinical question, with the radiologist involved.
- Metformin: for iodinated contrast, withhold metformin from the time of contrast and for 48 hours afterward if eGFR <60 (or a large contrast volume is used), resuming only after renal function is confirmed stable (ESUR guidance). This prevents metformin accumulation and lactic acidosis if CA-AKI occurs.
- Allergy / prior reaction: a previous severe (anaphylactoid) reaction to iodinated contrast is a red flag requiring premedication or an alternative study; document it and involve the radiologist.
- Gadolinium and the kidney: for MRI contrast, check eGFR; at eGFR <30 avoid gadolinium or use a macrocyclic agent only, because of nephrogenic systemic fibrosis risk.
- MRI device/foreign-body screening: a positive answer for a pacemaker/ICD, cochlear implant, aneurysm clip or possible intra-ocular metal is a STOP — do not enter the magnet room until the specific device is confirmed MRI-conditional or the foreign body is excluded (orbital X-ray).
- Pregnancy: exclude pregnancy before any ionising study (X-ray, fluoroscopy, CT, IVU) in a woman of reproductive age; if confirmed or possible, reconsider a non-ionising alternative (USG/MRI).
Provided image
SELF-CHECK
A 64-year-old man on metformin is booked for a contrast-enhanced CT abdomen. His eGFR is 52 mL/min/1.73 m². How should his metformin be managed according to standard (ESUR) guidance?
A. Continue metformin as normal; an eGFR of 52 needs no change
B. Withhold metformin from the time of contrast and for 48 hours after, resuming only once renal function is confirmed stable
C. Stop metformin permanently before any future contrast study
D. Switch metformin to insulin for one week before the scan
Reveal Answer
Answer: B. Withhold metformin from the time of contrast and for 48 hours after, resuming only once renal function is confirmed stable
ESUR guidance advises withholding metformin from the time of iodinated contrast administration and for 48 hours afterward in patients with eGFR <60 (or when a large contrast volume is given), resuming only after renal function is confirmed stable. This avoids metformin accumulation and lactic acidosis if contrast-associated AKI develops. An eGFR of 52 is below 60, so 'continue as normal' is wrong. Permanent discontinuation and a week of insulin substitution are not standard guidance.
Applied Practice — Worked Patient-preparation Scenarios
The skill of RD6.1 is best consolidated by working through realistic referrals and constructing, for each, the correct tailored written-and-verbal instruction set. Read each scenario and decide what you would write on the patient's sheet and what you would say before the patient leaves your consultation — including any safety screening you must arrange and any red flag you must check at the door. Then compare your plan with the worked answer. Notice that in every case the instruction is built from the same disciplined reasoning: first identify the goal (is this preparation protecting image quality or patient safety?), then select the procedure-specific preparation that serves that goal, and finally deliver it in both written and verbal channels and confirm it with a teach-back check. The cases below deliberately span the common situations you will meet: a patient whose medication must be adjusted, a patient in whom the modality itself must be reconsidered, a patient who needs detailed bowel preparation at home, and a patient whose occupation creates a hidden safety hazard. Train yourself to construct the sheet rather than recall one.
- Scenario 1 — Diabetic for contrast CT. A 60-year-old man with type 2 diabetes on metformin needs a contrast-enhanced CT abdomen for suspected malignancy. Plan: arrange/confirm a recent eGFR; if eGFR <60, instruct him in writing and verbally to withhold metformin from the time of contrast and for 48 hours afterward, resuming after renal review; ask about prior contrast reaction; advise good oral hydration and a light 4-hour fast; give the date, time, location and contact number. At the door, verify the eGFR value and that metformin was handled.
- Scenario 2 — Pregnant woman needing abdominal imaging. A 28-year-old at 10 weeks' gestation has right-upper-quadrant pain. Plan: choose ultrasound (no ionising radiation); instruct her to fast 4–6 hours for gallbladder assessment; reassure her that ultrasound is safe in pregnancy; avoid CT/iodinated contrast unless unavoidable. Written + verbal, with teach-back.
- Scenario 3 — Barium enema. A 55-year-old needs a barium enema for altered bowel habit. Plan: written instructions for a low-residue diet for 1–2 days, the prescribed laxative the evening before, a cleansing enema as directed, and fasting on the morning; warn about chalky-white stools and the need to hydrate to prevent constipation; verbally confirm she understands the laxative timing.
- Scenario 4 — Possible intra-ocular metal before MRI. A 40-year-old welder needs an MRI brain. Plan: complete the MRI safety questionnaire; because of the occupational risk of an intra-ocular ferromagnetic foreign body, arrange an orbital X-ray before the MRI; instruct him to remove all metal objects; declare any implants. At the door, do not proceed until the orbital screen is clear.
Working cases this way turns a memorised list into a transferable reasoning skill: you are never reciting a sheet, you are constructing the right sheet for this patient and this procedure.
SELF-CHECK
A 35-year-old woman is referred for an MRI of the lumbar spine for sciatica. During preparation, she mentions she had a cardiac pacemaker fitted two years ago. What is the correct action before she enters the MRI room?
A. Proceed; pacemakers are no longer a concern with modern MRI scanners
B. Do not proceed until the specific device is confirmed to be MRI-conditional and the manufacturer's protocol is followed (or choose an alternative)
C. Proceed but scan at a higher field strength to overcome the device
D. Remove the pacemaker before the scan
Reveal Answer
Answer: B. Do not proceed until the specific device is confirmed to be MRI-conditional and the manufacturer's protocol is followed (or choose an alternative)
A cardiac pacemaker is a critical MRI safety screening item and a STOP until cleared. MRI may proceed only if the specific device is confirmed MRI-conditional and the manufacturer's protocol (field strength, programming, monitoring) is followed; otherwise an alternative (e.g. CT) is used. Assuming all pacemakers are safe is dangerous, higher field strength increases rather than reduces the risk, and removing the device is not an option. This is exactly the kind of red flag the pre-procedure check is designed to catch.
CLINICAL PEARL
Pearl 1 — Always give instructions in BOTH channels. Verbal counselling lets you confirm understanding (teach-back) and answer questions in the patient's language; the written sheet survives the journey home and carries the date, time, location and a contact number. One without the other is a half-done instruction — RD6.1 explicitly requires both.
Pearl 2 — Know which ultrasound needs a FULL bladder and which needs an EMPTY one. Transabdominal pelvic/obstetric scans need a FULL bladder (acoustic window); transvaginal scans need an EMPTY bladder; abdominal (gallbladder) scans need FASTING, not bladder filling. Telling a transvaginal patient to drink and hold is a common, avoidable error.
Pearl 3 — 'No eGFR on the form' = 'unknown eGFR', not 'normal eGFR'. Never inject iodinated contrast assuming renal function is fine because nobody wrote it down. Obtain the value first; an unknown renal function is itself a red flag.
Pearl 4 — The MRI magnet is always on. Ferromagnetic screening is not a formality. A patient with a possible intra-ocular metal fragment (welders, grinders) needs an orbital X-ray before MRI; an unscreened pacemaker or aneurysm clip is a STOP.
Self-Assessment — Tailoring Instructions to Patient and Procedure
Use these scenario questions to test your ability to construct procedure-specific written and verbal instructions and to recognise the safety thresholds and red flags. Write your full instruction set before reading each discussion — including what you would write, what you would say, what screening you would arrange, and what you would check at the door.
Scenario A: A 70-year-old man with haematuria is referred for an intravenous urogram (IVU). He is on metformin for diabetes and his eGFR three months ago was 48. What preparation and safety instructions do you give?
Discussion: IVU uses iodinated contrast, so safety governs the preparation. Confirm an up-to-date eGFR (the 3-month-old value of 48 should be rechecked); because eGFR is <60, instruct him — in writing and verbally — to withhold metformin from the time of contrast and for 48 hours afterward, resuming after renal review. Advise good hydration and a light fast; ask about prior contrast reactions; exclude no pregnancy (male patient) but confirm identity, clinical question and consent. At the door, verify the current eGFR and that metformin was withheld.
Scenario B: A 26-year-old woman at 8 weeks' gestation has suspected gallstones. The intern has booked a CT abdomen. How do you correct and prepare this?
Discussion: CT is ionising and contrast-based — inappropriate as first-line here. Switch to ultrasound abdomen, which is safe in pregnancy and excellent for gallstones. Instruct her to fast 4–6 hours so the gallbladder distends; reassure her about safety; deliver written + verbal instructions with teach-back. No contrast or metformin issues apply.
Scenario C: A 58-year-old woman is booked for a barium enema for change in bowel habit. She asks what she needs to do at home. What do you tell her?
Discussion: Barium enema needs bowel preparation for image quality: a low-residue diet for 1–2 days, a prescribed laxative the evening before, and a cleansing enema as directed, with fasting on the morning of the study. Warn her that stools will be chalky-white for a day or two and that she should drink plenty of fluids to avoid constipation. Provide a written sheet and confirm verbally that she understands the laxative timing and the diet.
Scenario D: A 45-year-old metal-fabrication worker needs an MRI brain for headaches. What is the mandatory preparation step specific to his occupation?
Discussion: Complete the MRI safety questionnaire and, because of the occupational risk of an intra-ocular ferromagnetic foreign body, arrange an orbital X-ray to exclude metal fragments before the MRI. Instruct him to remove all metal objects and declare any implants. If metal is found in the eye, MRI is contraindicated and CT is the alternative. Do not enter the magnet room until the orbital screen is clear.