Page 7 of 14
RD3.4 | PC-PNDT Act for Primary Care Practice — SDL Guide
Learning Objectives
- State the full name, purpose and legislative history of the PC-PNDT Act 1994 (and its 2003 amendment).
- List the core prohibitions of the Act — sex selection, disclosure of foetal sex, and advertisement of sex-determination services.
- Distinguish the permitted uses of prenatal diagnostic techniques (detecting genetic/chromosomal/congenital abnormalities) from the prohibited use (sex determination).
- Describe the regulatory machinery: registration of clinics, mandatory Form F record-keeping, statutory signage, and the role of the Appropriate Authority.
- Apply the Act to the duties and pitfalls of a primary-care physician who refers for or performs obstetric ultrasound.
INSTRUCTIONS
This module addresses a legal and ethical obligation that every Indian doctor carries, regardless of specialty. The PC-PNDT Act exists to halt the misuse of diagnostic imaging — chiefly ultrasound — for prenatal sex determination and the sex-selective abortion that follows it, a practice that has skewed India's child sex ratio. Competency RD3.4 requires the primary-care physician to be knowledgeable about the purpose and components of this Act. Unlike the AERB radiation rules, this is not about dose; it is about preventing a social harm through legal regulation of imaging. Understanding it protects your patients, protects vulnerable female foetuses, and protects you from serious criminal liability.
References
- The Pre-Conception and Pre-Natal Diagnostic Techniques (Prohibition of Sex Selection) Act 1994 (as amended 2003), Government of India (guideline)
- PC-PNDT Rules 1996 (as amended), Ministry of Health and Family Welfare, Government of India (guideline)
- Reddy's The Essentials of Forensic Medicine and Toxicology — chapter on medical law and reproductive legislation (textbook)
- DC Dutta's Textbook of Obstetrics — prenatal diagnosis and the PC-PNDT Act (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A young woman comes to your primary-care clinic for a routine antenatal check at 18 weeks. After the consultation, her mother-in-law quietly draws you aside and asks, 'Doctor, when she has her scan, can you just tell us if it is a boy or a girl? We only want to prepare.' The request sounds innocent — even loving. But if you, or the radiologist you refer her to, answer that question, you will have committed a criminal offence under Indian law, regardless of intent, and you will have taken one small step on the road that has left India with millions of 'missing girls'. The misuse of ultrasound to identify and then abort female foetuses is not a rare aberration; it was once routine, advertised openly, and it bent the country's child sex ratio out of shape. A single Act of Parliament stands against it, and it places duties directly on you. This module is about that Act — what it forbids, how it works, and exactly what you, as a primary-care doctor, must and must not do.
WHY THIS MATTERS
Competency RD3.4 requires the primary-care physician to be knowledgeable about the purpose and components of the PC-PNDT Act relevant to practice. This matters for three concrete reasons. First, it is law with criminal penalties — a doctor who discloses foetal sex, or who runs an unregistered ultrasound facility, or who fails to keep the mandatory records faces imprisonment, fines and loss of registration. Second, it is an everyday clinical situation: requests to reveal foetal sex are common, often pressured, and you must know how to refuse them lawfully and compassionately. Third, it is a genuine public-health and ethical responsibility — the Act is society's chief instrument against sex-selective elimination of girls, and every compliant doctor is part of that defence. Examiners test the Act's full name, its prohibitions, the Form F requirement, and the distinction between permitted and prohibited prenatal diagnosis. More importantly, your conduct in clinic depends on knowing it cold.
RECALL
Before continuing, bring to mind a few facts that frame this Act:
- Ultrasound is the technique chiefly misused for sex determination: foetal external genitalia can often be identified on second-trimester ultrasound, which is precisely why USG clinics are the central target of regulation.
- Permitted prenatal diagnosis is a legitimate, valuable practice: techniques such as ultrasound, amniocentesis and chorionic villus sampling (CVS) are properly used to detect chromosomal disorders (e.g. Down syndrome), genetic and metabolic conditions, and structural congenital anomalies.
- The child sex ratio: the number of girls per 1000 boys in the 0–6 year age group has declined in successive Indian censuses — the demographic evidence of sex selection that the Act was written to reverse.
- This is distinct from radiation regulation: the AERB governs radiation dose; the PC-PNDT Act governs the social misuse of imaging and applies even though ultrasound uses no ionising radiation at all.
- Law applies regardless of intent: a 'harmless' disclosure of foetal sex is still an offence.
Holding these in mind will make the prohibitions and the doctor's duties below follow logically.
Orientation — Why a Radiology Act Concerns Every Primary-Care Doctor
It may seem surprising that a competency in radiodiagnosis concerns a social-justice statute rather than imaging physics, but the connection is direct and important. Diagnostic imaging is a powerful technology, and like any powerful technology it can be turned to harmful ends. In the Indian context the most consequential misuse of imaging has not been a question of radiation dose at all, but the use of ultrasound to identify the sex of a foetus so that female foetuses could be selectively aborted. This practice, driven by deep-rooted son preference, became widespread once portable ultrasound made foetal sexing cheap and easy, and its cumulative effect distorted the population's child sex ratio to a degree visible in national census data. A primary-care physician who refers women for obstetric ultrasound, or who performs it, is therefore positioned at the very point where this misuse occurs — which is exactly why the law places duties on the ordinary clinician and not only on specialist radiologists.
The regulatory response operates differently from the radiation framework you have studied:
- The AERB / ALARA framework controls a physical hazard (radiation dose) through justification, optimisation and dose limits.
- The PC-PNDT Act controls a social hazard (sex-selective elimination of girls) by prohibiting the misuse of diagnostic techniques and regulating who may perform them and how they must be documented.
Both are 'radiation safety and legal requirements' in the broad sense the curriculum intends, but they protect against entirely different harms. The PC-PNDT Act reaches you because the technique it regulates — ultrasound — is one you will routinely order and because the request to misuse it will be made to you directly.
PC-PNDT Act: Mandatory Signage and Social Purpose
The PC-PNDT Act 1994 — Purpose, Scope and Core Prohibitions
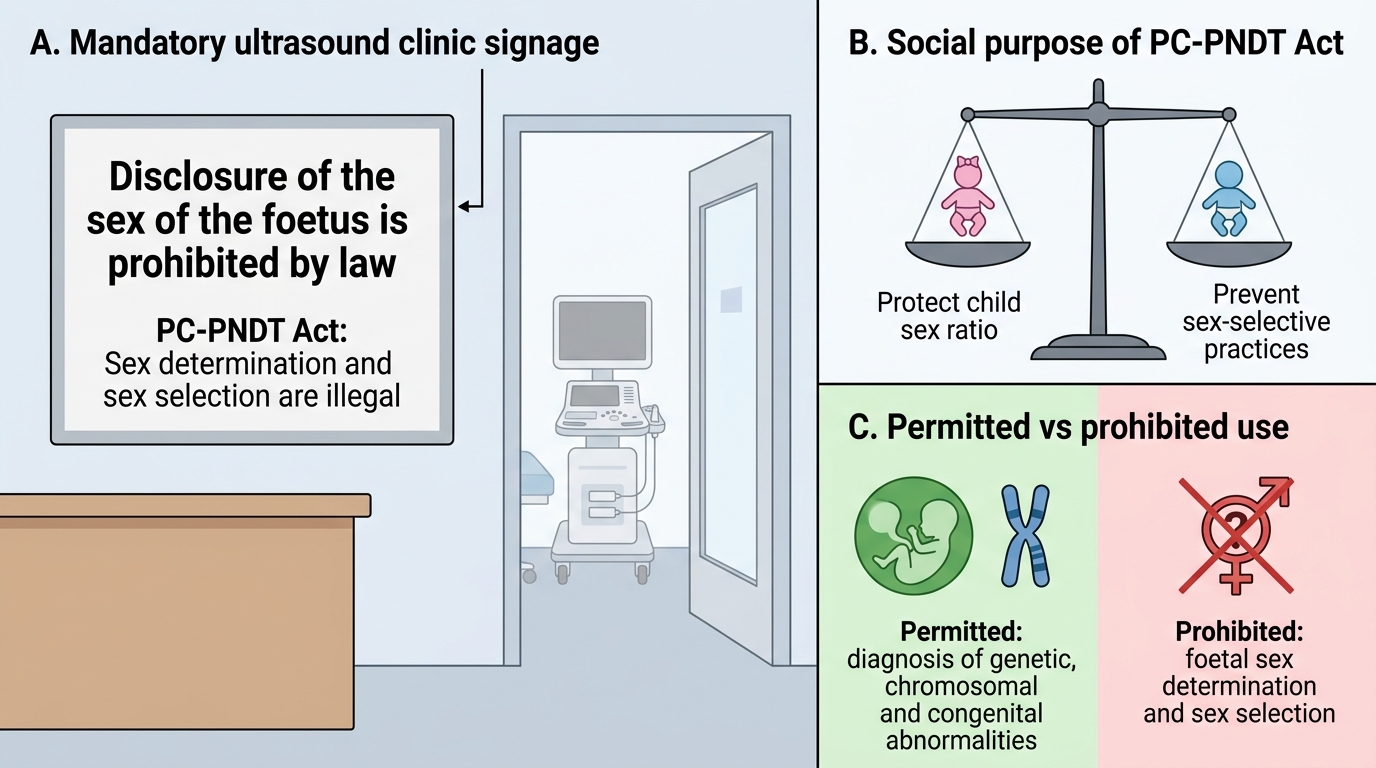
The Act's full title tells you most of what it does: the Pre-Conception and Pre-Natal Diagnostic Techniques (Prohibition of Sex Selection) Act. It was originally enacted in 1994 as the Pre-Natal Diagnostic Techniques (PNDT) Act and came into force in 1996; a significant amendment in 2003 broadened its reach to cover pre-conception sex-selection techniques (such as sperm sorting) and to tighten regulation, after which it became known as the PC-PNDT Act. Its single overriding purpose is to prohibit sex selection and prevent the misuse of prenatal diagnostic techniques for the determination of foetal sex, thereby arresting the decline in the child sex ratio. It is essential to be precise about what the Act forbids and what it deliberately permits, because the legitimate, life-saving uses of prenatal diagnosis must continue while only the harmful use is stopped.
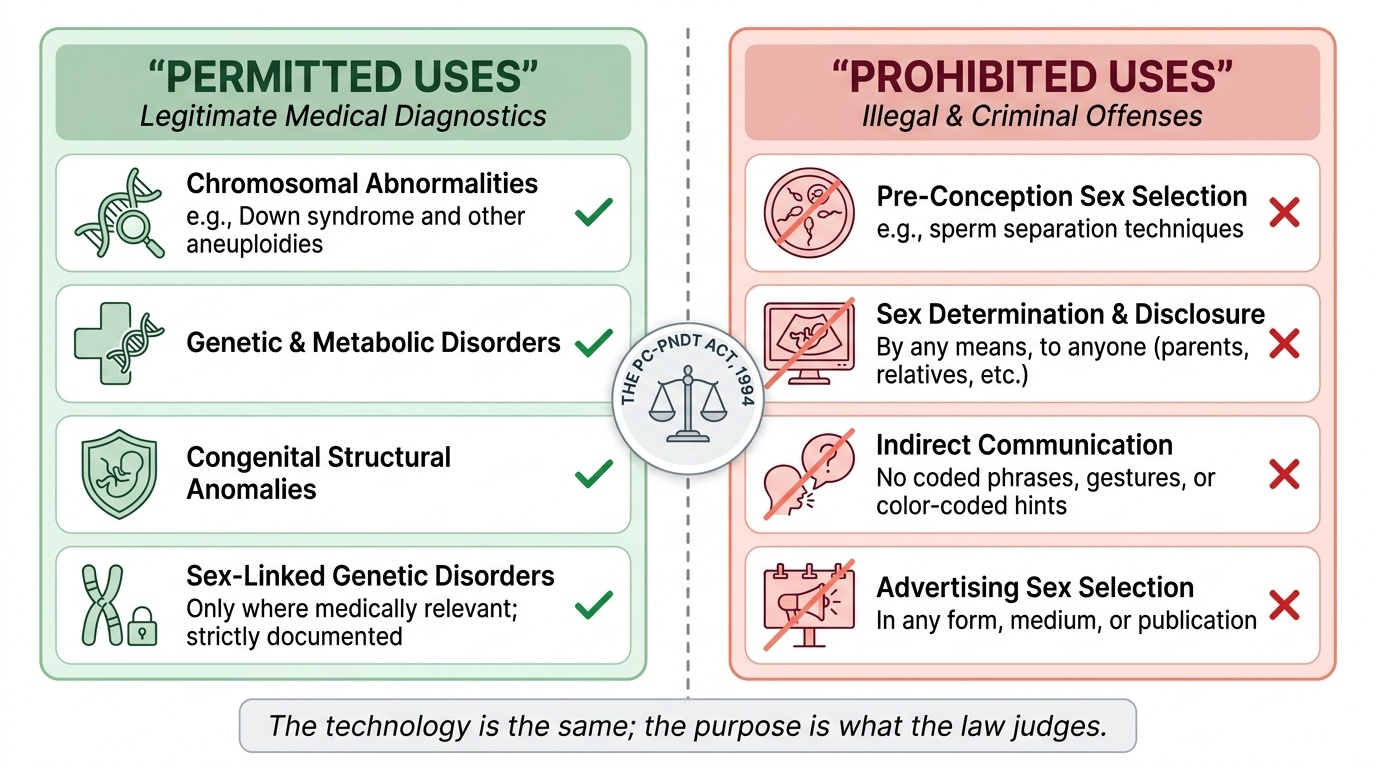
The Act's core prohibitions are:
- No sex selection of any kind, whether pre-conception (e.g. sperm separation techniques) or pre-natal.
- No determination or disclosure of the sex of the foetus — by any means, to anyone (the pregnant woman, her relatives, or anyone else). Even an indirect communication (a gesture, a coded phrase, a colour) is prohibited.
- No advertisement relating to pre-natal/pre-conception sex determination or sex selection, in any form or medium.
Equally important is what the Act permits. Prenatal diagnostic techniques (ultrasound, amniocentesis, chorionic villus sampling, foetal blood sampling, genetic testing) remain fully legal when used for their proper medical purpose — detecting:
- Chromosomal abnormalities (e.g. Down syndrome and other aneuploidies),
- Genetic and metabolic disorders,
- Congenital structural anomalies, and certain sex-linked genetic disorders (where knowing the sex may be medically relevant — handled under strict, documented conditions, never for selection).
Thus the Act draws a sharp line: prenatal diagnosis to detect disease is permitted and encouraged; prenatal diagnosis to determine sex for selection is criminal. The technology is the same; the purpose is what the law judges.
Provided image
SELF-CHECK
A primary-care doctor refers a 35-year-old pregnant woman for amniocentesis because of a high-risk screening result for Down syndrome. The laboratory karyotype incidentally reveals the foetal sex. Under the PC-PNDT Act, what is the correct handling?
A. The sex may be disclosed to the parents because the test was performed for a legitimate medical reason
B. The chromosomal analysis for Down syndrome is a permitted use, but the foetal sex must NOT be disclosed to the woman or her relatives by any means
C. The amniocentesis itself is illegal under the Act because it can reveal foetal sex
D. Disclosure is permitted as long as it is recorded in Form F
Reveal Answer
Answer: B. The chromosomal analysis for Down syndrome is a permitted use, but the foetal sex must NOT be disclosed to the woman or her relatives by any means
Using amniocentesis to detect a chromosomal abnormality such as Down syndrome is a fully PERMITTED use of prenatal diagnosis — the technique and the indication are legitimate. However, the Act's prohibition on DISCLOSING foetal sex is absolute and applies regardless of how the sex became known: even when sex is revealed incidentally during a legitimate test, it must NOT be communicated to the woman or her relatives by any means. The test is not illegal (option 3 is wrong), and Form F documents compliance but never licenses disclosure (option 4 is wrong).
How the Act Works — Registration, Form F, Signage and Authorities
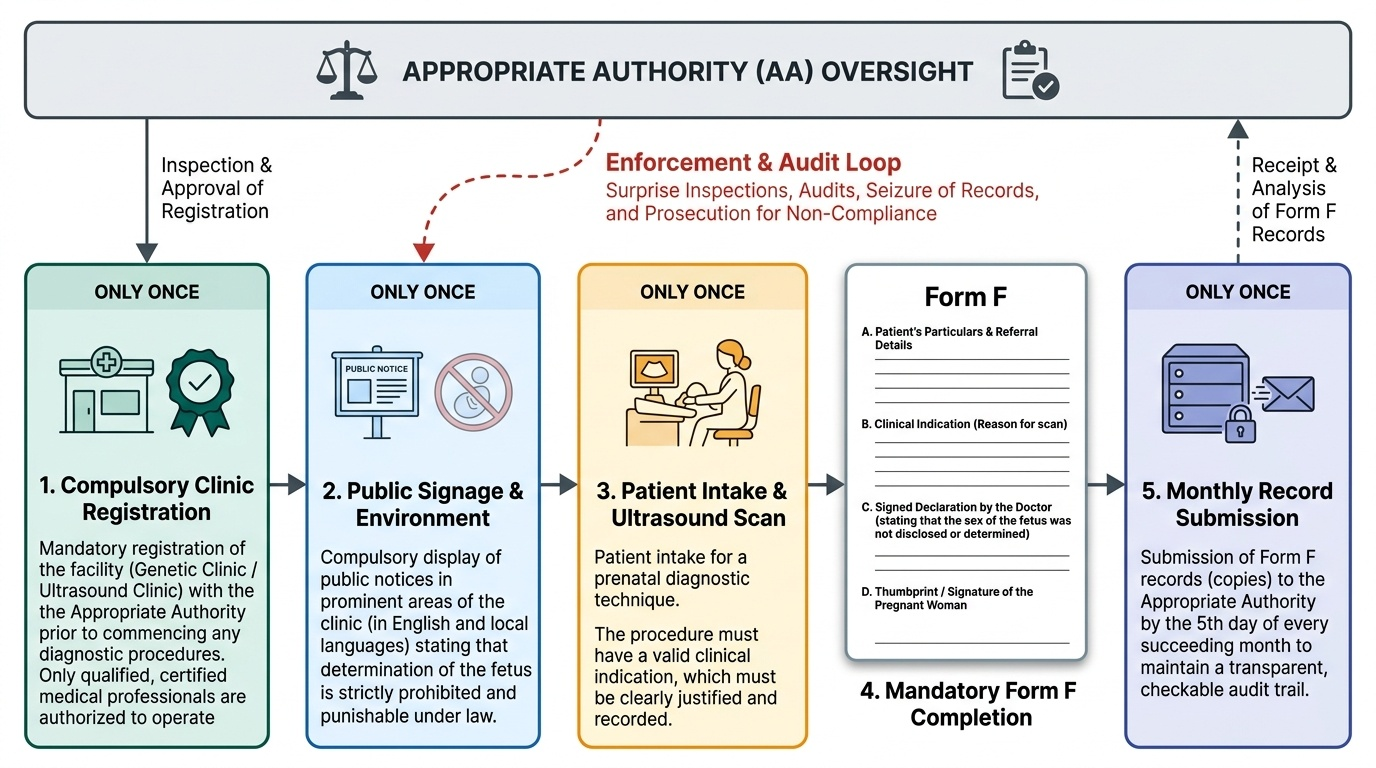
Prohibitions alone do not stop a hidden practice, so the Act deliberately backs its rules with a whole machinery of registration, documentation, public signage and enforcement authorities. Understanding this machinery is what turns the bare statement 'the Act forbids sex determination' into a concrete set of obligations that a clinic and an individual doctor must actually fulfil in everyday work, and it is the part of the competency most often tested in detail because each component is a discrete, checkable, auditable requirement rather than a vague principle. The design of the system is deliberate and mutually reinforcing: by registering every facility, documenting every single scan on a prescribed form, displaying a public notice, and empowering a local authority to inspect and prosecute, the Act makes covert sex determination far harder to carry out and creates a clear paper trail to follow whenever a violation is suspected.
The key components of the operating machinery are:
- Compulsory registration: every genetic counselling centre, genetic laboratory, genetic clinic and ultrasound/imaging clinic that uses prenatal diagnostic techniques must be registered with the Appropriate Authority. No such facility may operate without registration, and only qualified persons (with prescribed qualifications) may conduct the procedures.
- Mandatory Form F: for every pregnant woman undergoing an ultrasound or other prenatal diagnostic procedure, the clinic must complete and maintain Form F — a detailed record capturing the woman's particulars, the clinical indication for the scan, and a signed declaration by the doctor that the sex of the foetus was not detected or disclosed. These records must be preserved and are submitted/available for inspection. Incomplete or improperly filled Form F is itself an offence and is one of the commonest grounds for prosecution.
- Statutory signage: registered facilities must prominently display a notice stating that determination/disclosure of the sex of the foetus is prohibited by law and not done at that centre.
- Appropriate Authority and Advisory Committee: the Act creates an Appropriate Authority (at district and state level) empowered to register and inspect facilities, seize records and equipment, and initiate prosecution, advised by an Advisory Committee.
- Penalties: contravention attracts criminal penalties — for a first offence, imprisonment up to 3 years and a fine up to Rs 10,000; for a subsequent offence, imprisonment up to 5 years and a fine up to Rs 50,000 — together with suspension or cancellation of registration and, for a registered medical practitioner, reporting to the Medical Council for action against registration.
Together these components create a regime in which performing prenatal imaging is legal and routine, but doing so without registration, without proper Form F records, or in a way that determines or discloses sex, is detectable and punishable.
Provided image
SELF-CHECK
Which document must a registered ultrasound clinic complete for EVERY pregnant woman undergoing a prenatal ultrasound, recording the clinical indication and a declaration that foetal sex was not disclosed?
A. Form A (the facility's registration certificate)
B. Form F
C. The AERB eLORA registration form
D. Form H (a voluntary consent form)
Reveal Answer
Answer: B. Form F
Form F is the mandatory record under the PC-PNDT Act that must be completed for every pregnant woman undergoing a prenatal ultrasound or diagnostic procedure. It documents the woman's particulars, the clinical indication for the scan, and a signed declaration by the doctor that the foetal sex was not determined or disclosed. Improperly maintained Form F records are one of the commonest grounds for prosecution. The facility's registration is a different document; the AERB eLORA form relates to RADIATION (and ultrasound is non-ionising, so it is not an AERB matter); 'Form H' is not the relevant statutory record here.