Page 1 of 4
AN40.1-5 | Organs of hearing and equilibrium — SDL Guide
Learning Objectives
- Describe and identify the parts, blood supply, and nerve supply of the external ear (AN40.1)
- Describe and demonstrate the boundaries, contents, relations, and functional anatomy of the middle ear and auditory tube (AN40.2)
- Describe the features of the internal ear — bony and membranous labyrinths (AN40.3)
- Explain the anatomical basis of otitis externa and otitis media and their complications (AN40.4)
- Explain the anatomical basis of myringotomy — site, rationale, and structures at risk (AN40.5)
INSTRUCTIONS
This module covers the three parts of the ear systematically. Pay close attention to the clinical correlations — ear disease is extremely common in Indian primary care practice.
References
- Gray's Anatomy for Students (Drake et al.) — Chapter 8: Head and Neck (Textbook)
- BD Chaurasia's Human Anatomy, Vol. 3 — Head & Neck (Textbook)
- Dhingra's Diseases of Ear, Nose and Throat (Textbook)
- OpenStax Anatomy and Physiology 2e — Special Senses (Open Access)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 9-year-old child from a village near Vellore is brought to the PHC with a 3-day history of severe right ear pain, fever, and fluid leaking from the right ear. The doctor at the PHC diagnoses acute otitis media with tympanic membrane perforation. She considers referring the child to the district hospital for myringotomy.
Where exactly is the tympanic membrane located? Why does infection spread so easily from the throat to the middle ear? Why is myringotomy performed in the anteroinferior quadrant and not the posterosuperior?
Understanding the anatomy of the ear will answer each of these questions — and will be essential every time you use an otoscope in clinical practice.
WHY THIS MATTERS
Ear anatomy is directly relevant to your clinical practice from Day 1 of MBBS clinical postings:
- Otitis media is the second most common reason for antibiotic prescription in Indian children; acute and chronic forms cause hearing loss and serious intracranial complications
- Otoscopy — examining the tympanic membrane — is a fundamental clinical skill that requires knowledge of the anatomy of the external auditory meatus
- Myringotomy and grommets — one of the most common paediatric surgical procedures; requires exact anatomical knowledge of the safe quadrant
- Facial nerve injury — the facial nerve (CN VII) runs through the middle ear; chronic otitis media and mastoiditis can damage it causing facial palsy
- Referred otalgia — ear pain from distant sites (throat cancer, temporomandibular joint, tonsillitis) via Arnold's nerve (CN X), Jacobson's nerve (CN IX), and auriculotemporal nerve (CN V3)
RECALL
Before we begin, recall:
- The temporal bone is one of the most complex bones in the body — it contains the middle ear cavity (tympanic cavity), mastoid air cells, internal auditory meatus, and the bony labyrinth of the inner ear
- The facial nerve (CN VII) enters the internal auditory meatus and passes through the petrous temporal bone, exiting at the stylomastoid foramen
- Sensory innervation of the auricle involves multiple nerves: great auricular (C2,C3), lesser occipital (C2), auriculotemporal (CN V3), and Arnold's nerve (auricular branch of CN X)
- Endolymph fills the membranous labyrinth; perilymph fills the space between bony and membranous labyrinths
Part 1: External Ear — Parts, Blood Supply, Nerve Supply (AN40.1)
The External Ear

Figure: External Auditory Meatus (EAM)

Figure: Part 1: External Ear — Parts, Blood Supply, Nerve Supply (AN40.1)
The external ear consists of:
1. Auricle (pinna) — cartilaginous (elastic cartilage) framework covered by perichondrium and skin
2. External auditory meatus (EAM) — S-shaped canal from the concha to the tympanic membrane
Auricle — Surface Anatomy
Key landmarks of the auricle:
• Helix — outer curved rim
• Antihelix — inner curved ridge parallel to helix; bifurcates superiorly into two crura
• Scapha — groove between helix and antihelix
• Concha — deep concavity leading to the EAM
• Tragus — small projection anterior to the meatus (used for pressing to occlude EAM)
• Antitragus — projection opposite to tragus
• Lobule — inferior soft tissue portion (no cartilage); site of ear piercing and earlobe keloids
External Auditory Meatus (EAM)
Length: approximately 2.5 cm in adults. Comprises:
• Outer 1/3: Cartilaginous (continuation of auricular cartilage); contains ceruminous (wax-secreting) glands and hair follicles
• Inner 2/3: Bony (formed by the tympanic plate of temporal bone)
The meatus has an S-shape. To straighten it for otoscopy:
• In adults: pull the pinna upward, backward, and laterally
• In children under 3: pull the pinna downward and backward (the meatus is shorter and more horizontal)
Blood Supply of External Ear:
• Posterior auricular artery (branch of external carotid) — posterior auricle and EAM
• Superficial temporal artery (branch of external carotid) — anterior auricle
• Anterior tympanic artery (branch of maxillary artery) — tympanic membrane
Nerve Supply of External Ear:
| Region | Nerve | Origin |
|---|---|---|
| Anterior auricle and anterior EAM | Auriculotemporal nerve | CN V3 (mandibular) |
| Posterior auricle | Greater auricular nerve | C2, C3 (cervical plexus) |
| Posterior EAM and adjacent auricle | Arnold's nerve (auricular branch of vagus) | CN X |
| Concha | Lesser occipital nerve (C2) + facial nerve (CN VII, small branch) | C2 + CN VII |
Clinical note: Arnold's nerve (CN X) in the EAM explains referred otalgia from the larynx, oesophagus, and even the heart (rare). It also explains the ear-cough reflex (Arnold's reflex) — coughing triggered by syringing the ear due to stimulation of the vagal branch. Additionally, posterior inferior myocardial infarction can rarely present with left-sided otalgia via vagal referred pain.
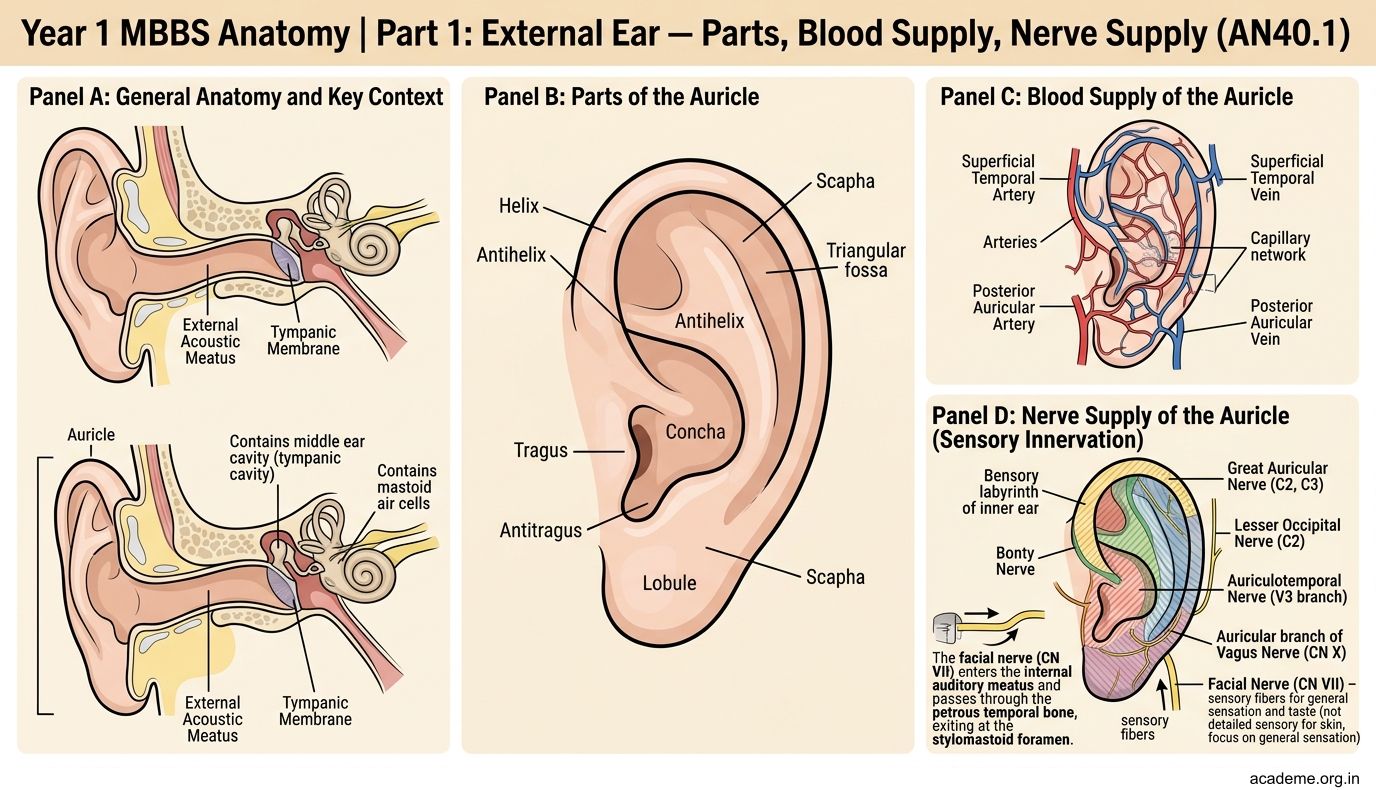
Figure: Part 1: External Ear — Parts, Blood Supply, Nerve Supply (AN40.1)

Figure: Auricle — Surface Anatomy
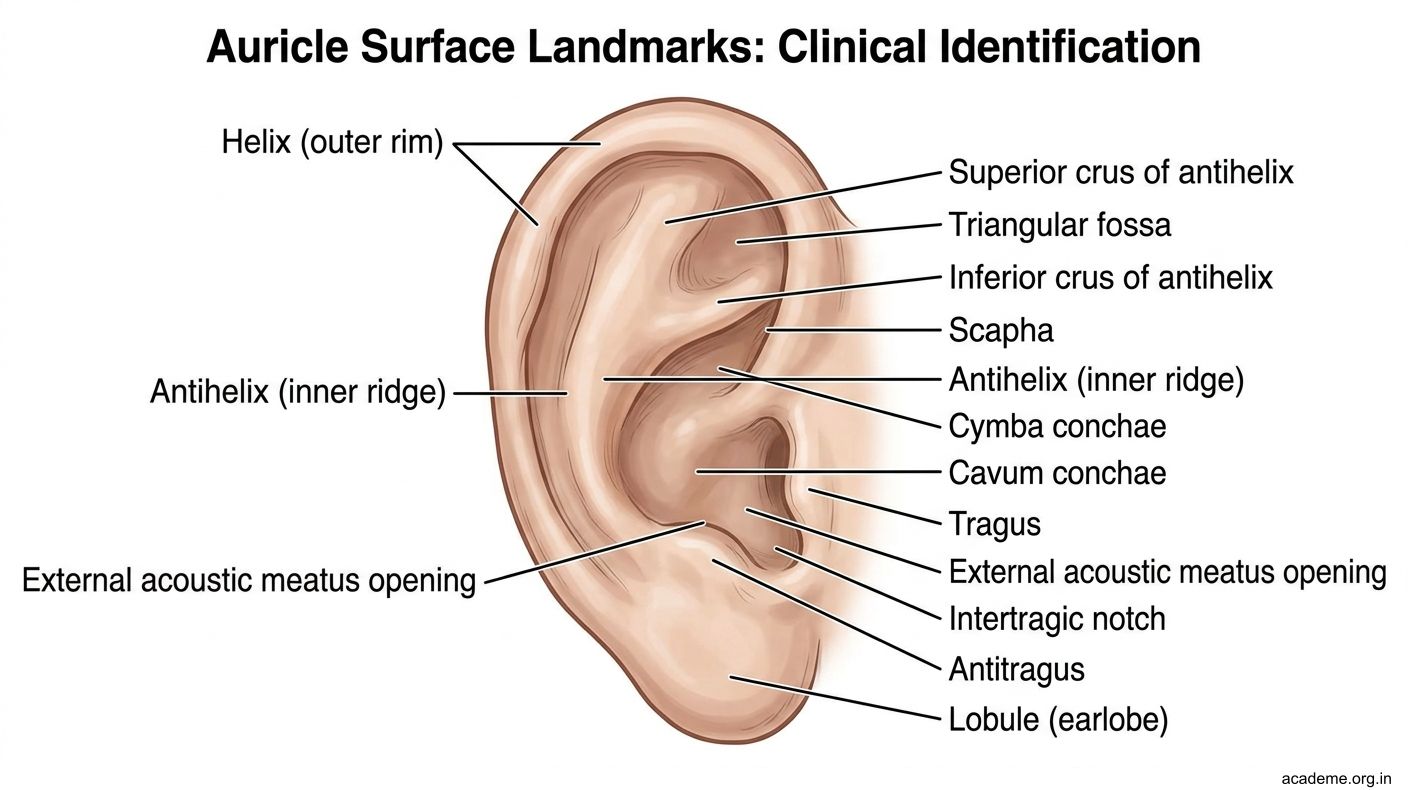
Figure: Auricle — Surface Anatomy
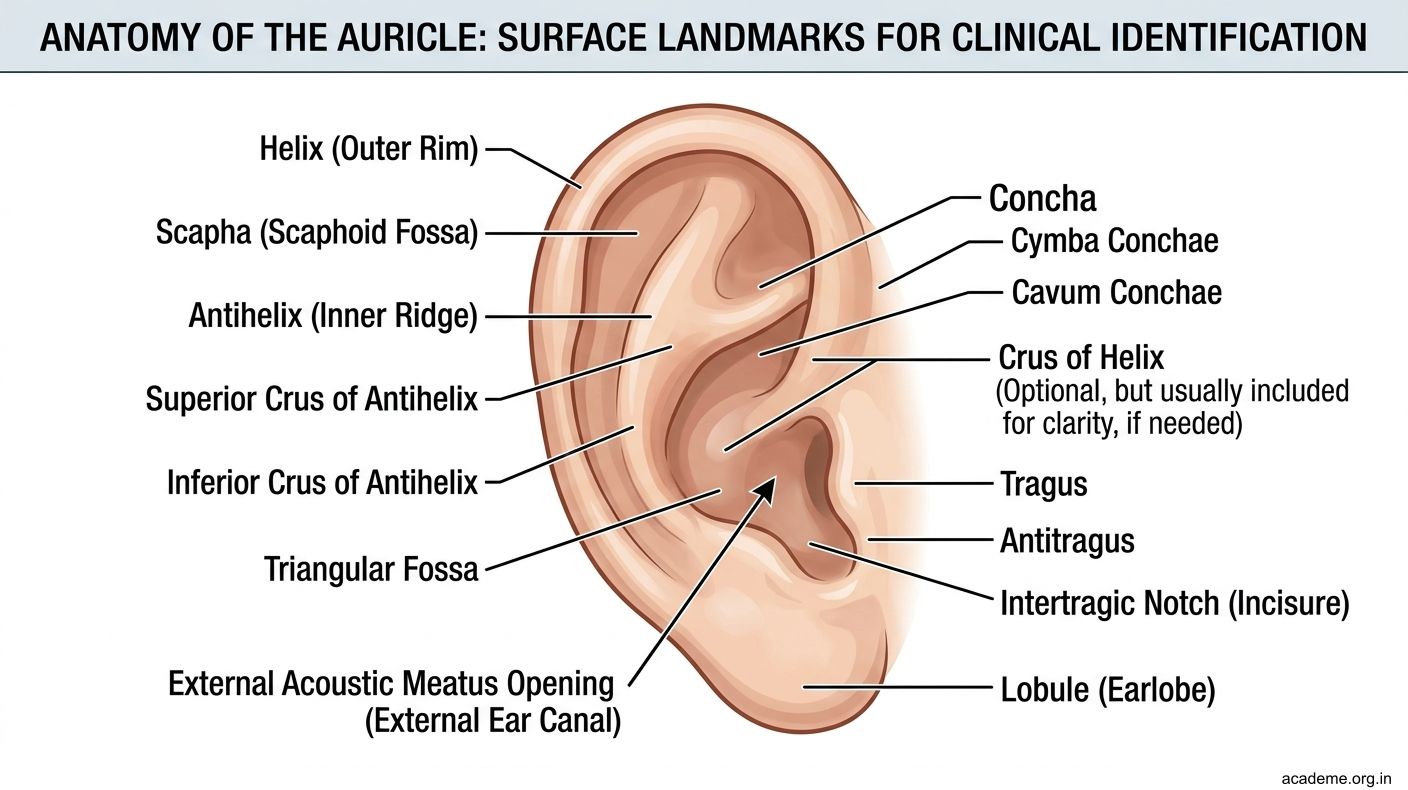
Figure: Auricle — Surface Anatomy
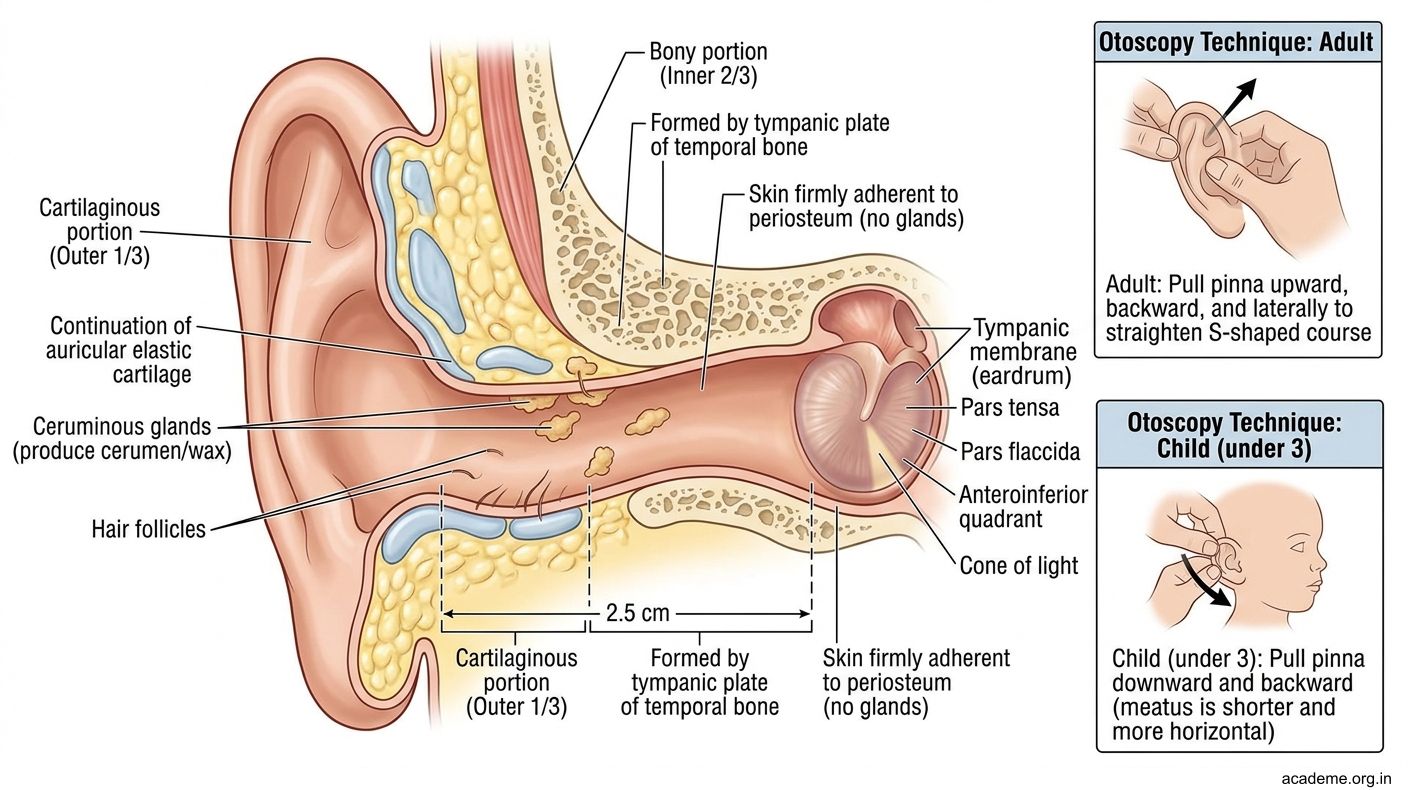
Figure: External Auditory Meatus (EAM)

Figure: Nerve Supply of External Ear:
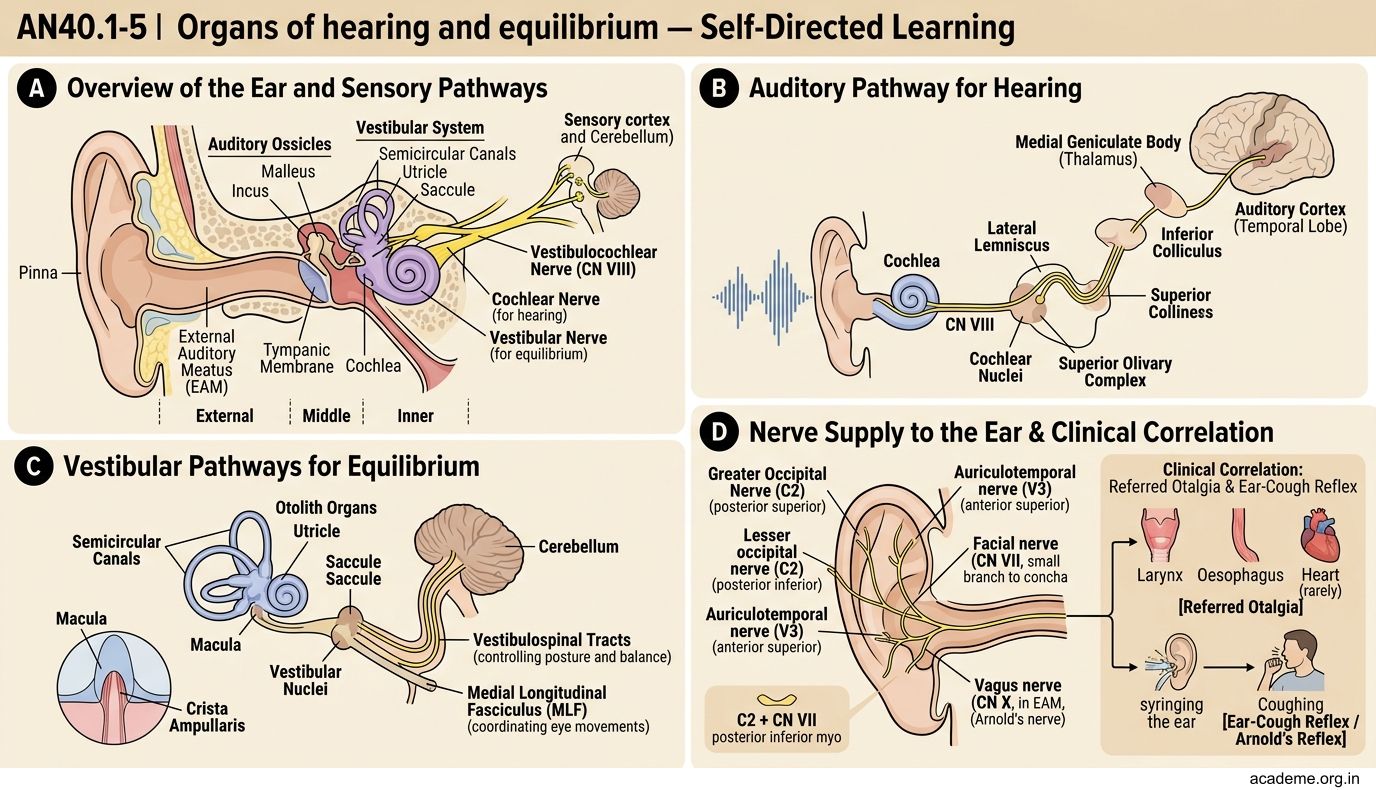
Figure: Nerve Supply of External Ear:
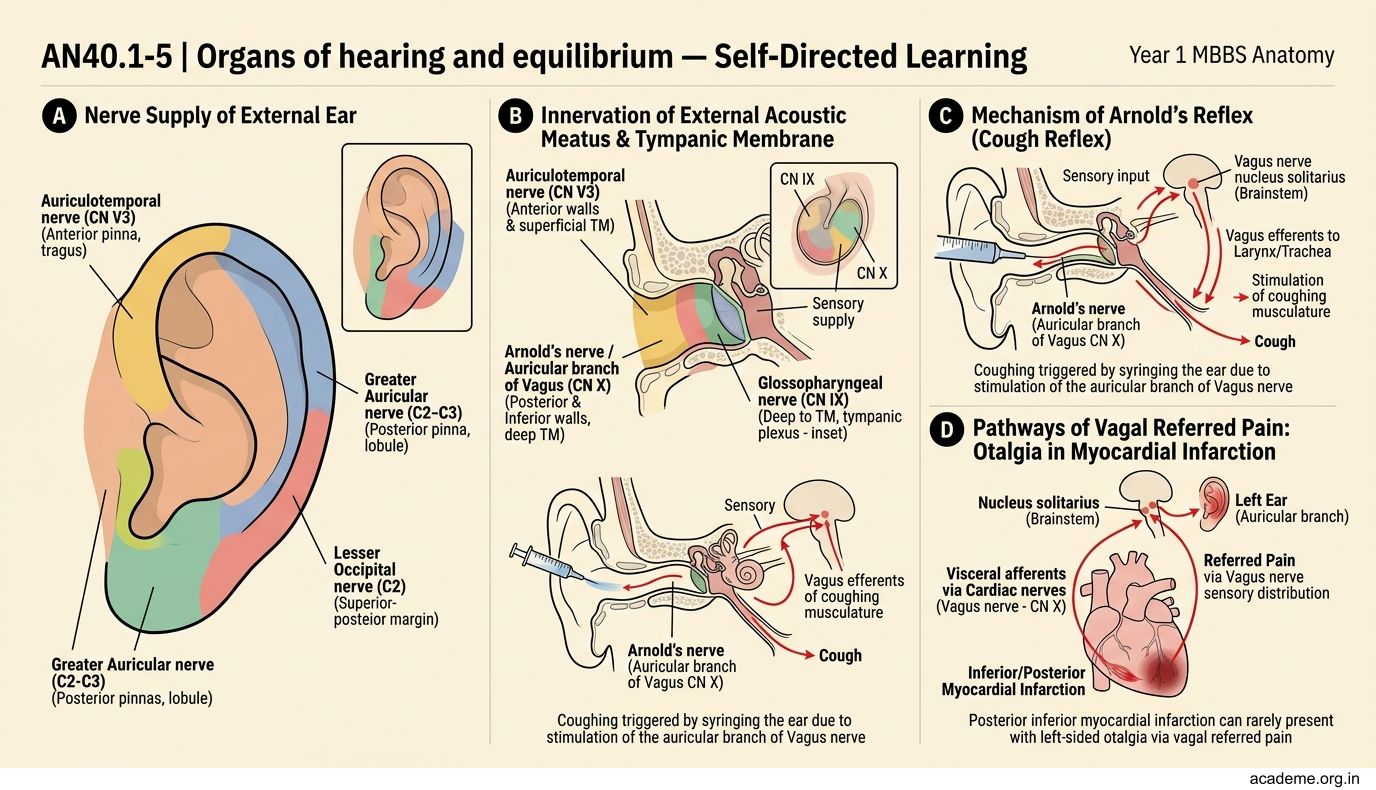
Figure: Nerve Supply of External Ear:
Part 2: Middle Ear and Auditory Tube (AN40.2)
Middle Ear (Tympanic Cavity)

Figure: Auditory (Eustachian) Tube (AN40.2)

Figure: Ossicles of the Middle Ear

Figure: Tympanic Membrane

Figure: Middle Ear (Tympanic Cavity)
The middle ear is an air-filled space within the petrous temporal bone. It is irregular in shape and described as having six walls:
| Wall | Also called | Key features |
|---|---|---|
| Lateral (membranous) wall | Tympanic wall | Tympanic membrane (eardrum) |
| Medial (labyrinthine) wall | Labyrinthine wall | Oval window (fenestra vestibuli) + Round window (fenestra cochleae) + Promontory (cochlea basal turn) + Facial nerve canal (horizontal part) |
| Anterior wall | Carotid wall | Opening of auditory (Eustachian) tube + tensor tympani canal; Internal carotid artery deep to this wall |
| Posterior wall | Mastoid wall | Aditus (opening to mastoid antrum) + Pyramid (contains stapedius muscle) |
| Roof (tegmental wall) | Tegmen tympani | Separates middle ear from middle cranial fossa; dura and brain above |
| Floor (jugular wall) | Jugular wall | Separates from internal jugular vein and jugular bulb below |
Tympanic Membrane
The eardrum is a semi-transparent, pearly grey membrane at approximately 55° angle. Divided into:
• Pars tensa (large lower part) — stretched, fibrous layer between outer squamous epithelium and inner mucosal layer
• Pars flaccida (Shrapnell's membrane) (small upper part above the lateral process of malleus) — no fibrous layer; more fragile
Otoscopic landmarks:
• Cone of light — triangular light reflex in the anteroinferior quadrant
• Handle of malleus — oblique ridge descending from the lateral process downward and backward
• Umbo — lowest point of malleus handle (deepest point of membrane)
Ossicles of the Middle Ear
Three tiny bones transmit vibration from the tympanic membrane to the oval window:
• Malleus (hammer) — handle embedded in tympanic membrane; head articulates with incus
• Incus (anvil) — body articulates with malleus; long process articulates with stapes
• Stapes (stirrup) — footplate covers the oval window; the smallest bone in the body
Muscles of the middle ear:
• Tensor tympani — supplied by CN V3 (medial pterygoid nerve); pulls malleus medially, tensing tympanic membrane
• Stapedius — supplied by CN VII (facial nerve); pulls stapes posteriorly, dampening oscillations
Clinical note: In Bell's palsy (facial nerve palsy), stapedius is paralysed → sounds appear abnormally loud (hyperacusis).
Auditory (Eustachian) Tube (AN40.2)
The auditory tube connects the nasopharynx to the anterior wall of the middle ear. Its function is to equalise pressure in the middle ear with atmospheric pressure.
- Length: approximately 36 mm (adults)
- Bony (medial 1/3) — lies in petrous temporal bone
- Cartilaginous (lateral 2/3) — opens into the nasopharynx at the torus tubarius
- Opens during swallowing and yawning via the levator palati and tensor palati muscles
Clinical relevance:
• In children, the tube is shorter, wider, more horizontal — allowing bacteria from the nasopharynx to reach the middle ear more easily → higher incidence of acute otitis media
• Adenoidal hypertrophy in children mechanically obstructs the tube → glue ear (otitis media with effusion)
• Cleft palate impairs tensor palati function → recurrent otitis media
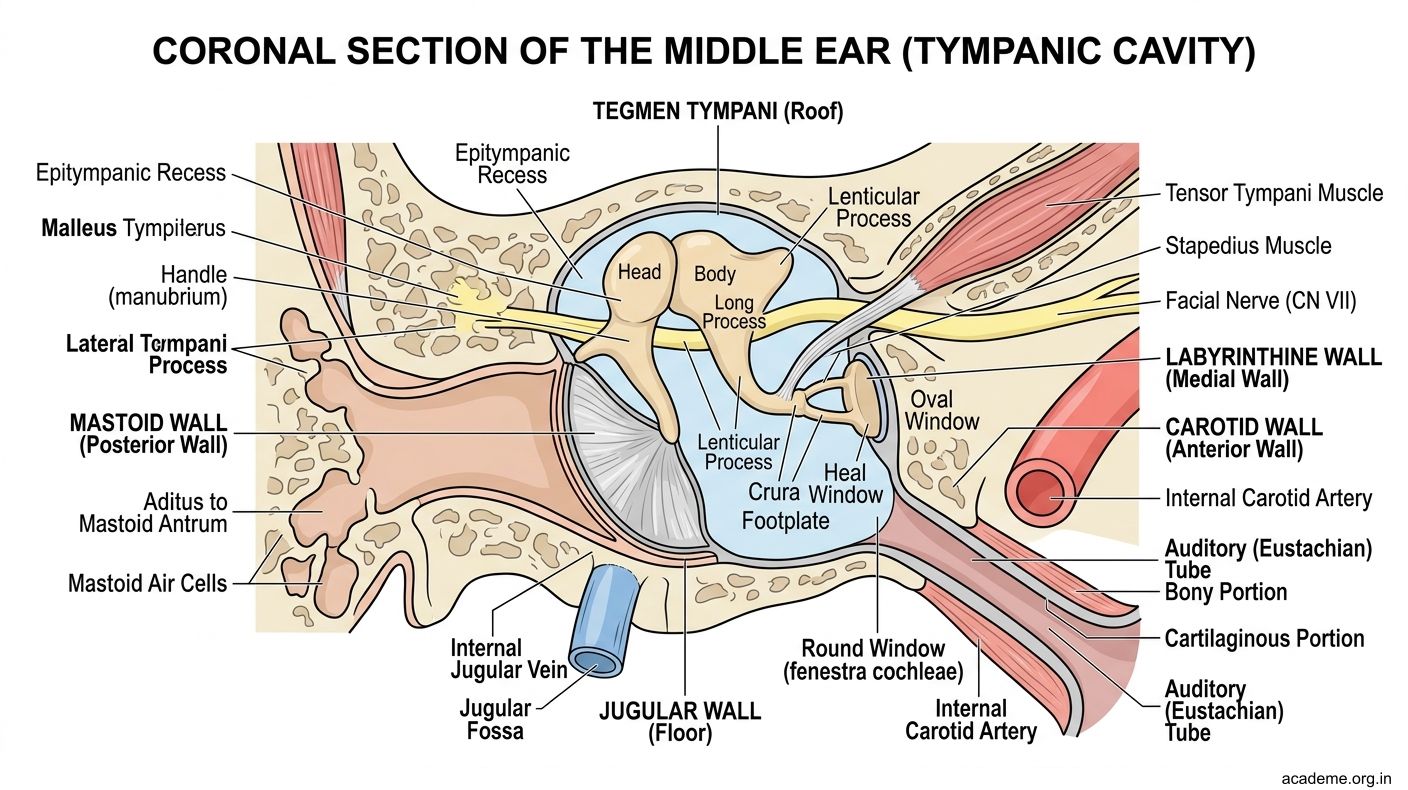
Figure: Part 2: Middle Ear and Auditory Tube (AN40.2)
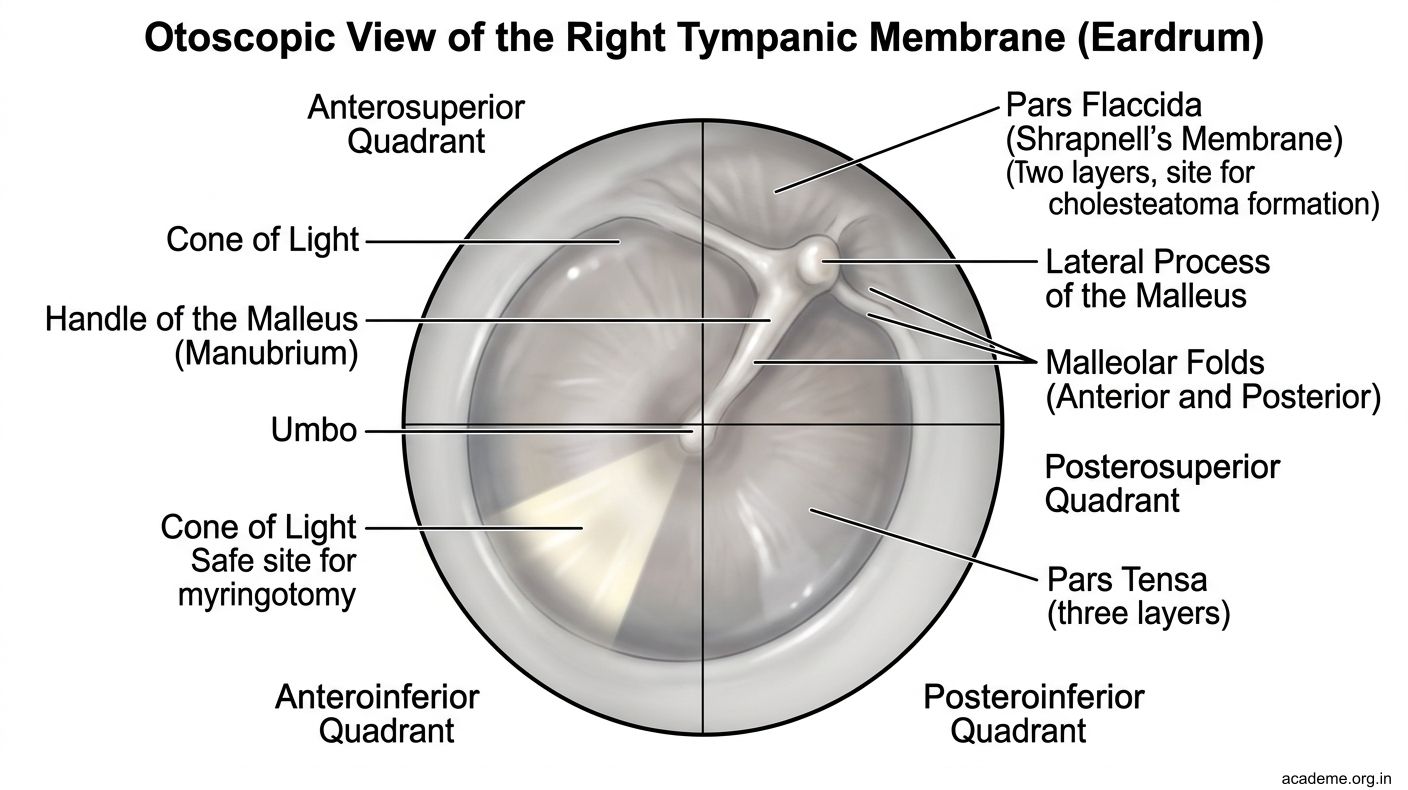
Figure: Tympanic Membrane
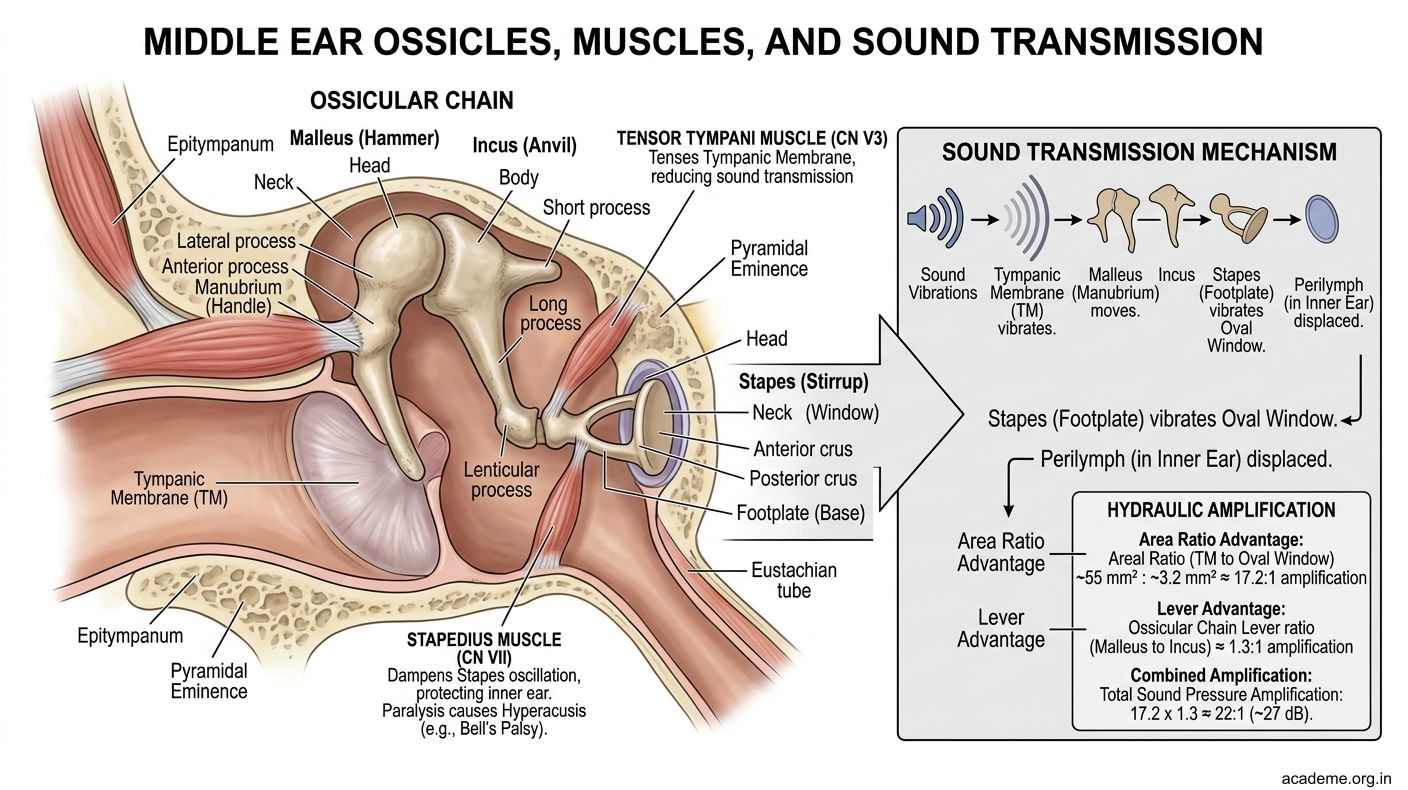
Figure: Ossicles of the Middle Ear
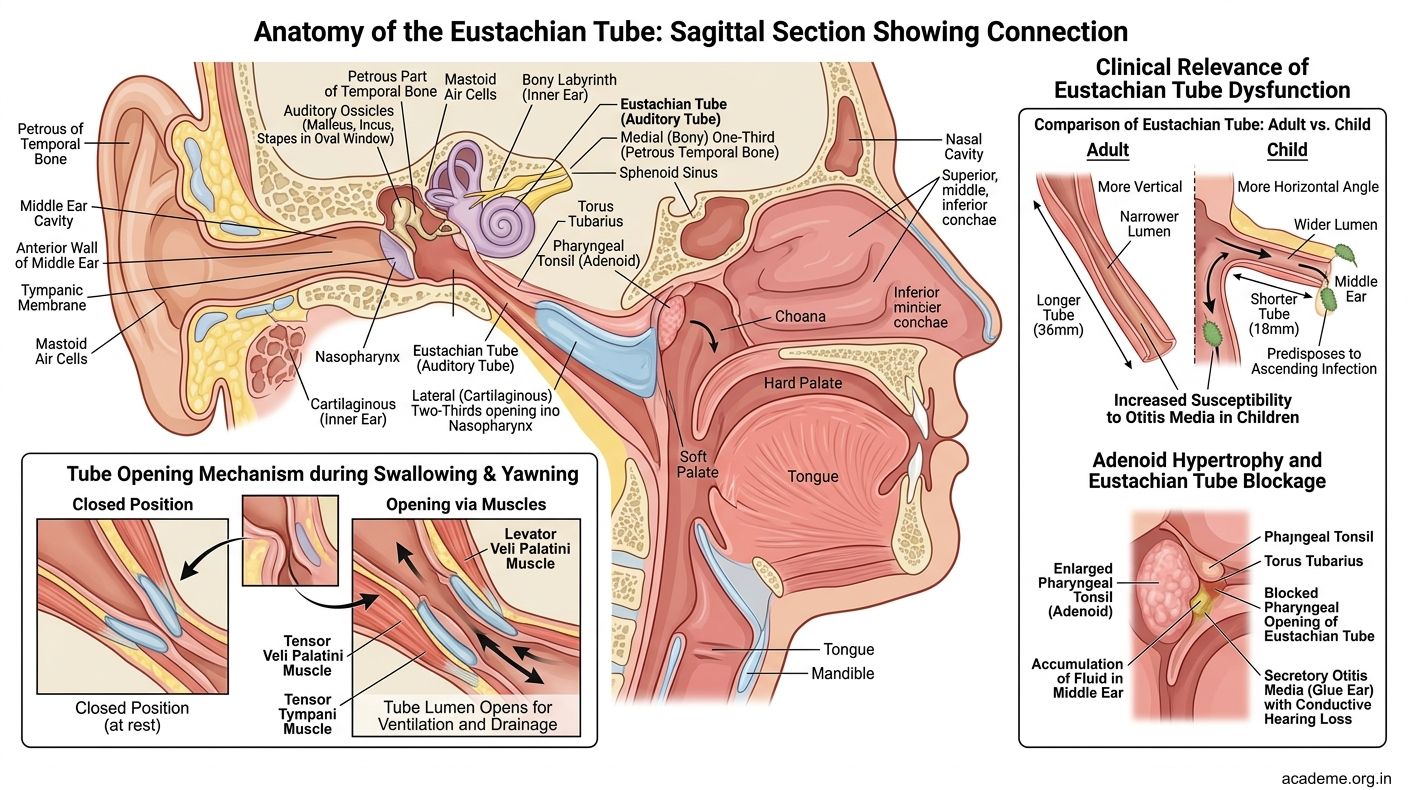
Figure: Auditory (Eustachian) Tube (AN40.2)
SELF-CHECK — : External and Middle Ear
Which nerve traverses the medial wall of the middle ear and is at risk in chronic suppurative otitis media causing facial palsy?
A. Tympanic nerve (CN IX)
B. Chorda tympani (CN VII)
C. Facial nerve (CN VII) in its horizontal canal
D. Auriculotemporal nerve (CN V3)
Reveal Answer
Answer: C. Facial nerve (CN VII) in its horizontal canal
A child presents with recurrent acute otitis media. The anatomical reason children are more susceptible than adults is:
A. Children have larger mastoid air cells
B. Children's auditory tube is shorter, wider, and more horizontal
C. Children have a thinner tympanic membrane
D. Children lack stapedius reflex
Reveal Answer
Answer: B. Children's auditory tube is shorter, wider, and more horizontal
Part 3: Internal Ear (AN40.3)
Internal Ear (Labyrinth)

Figure: Part 3: Internal Ear (AN40.3)
The internal ear consists of two parts:
1. Bony labyrinth — excavation in the petrous temporal bone; filled with perilymph (similar to CSF, ultrafiltrate of blood)
2. Membranous labyrinth — a closed membranous sac within the bony labyrinth; filled with endolymph (high K⁺, low Na⁺ — similar to intracellular fluid)
Bony Labyrinth — Three parts:
1. Cochlea (for hearing):
• Spiral canal of 2.5 turns around a bony pillar (modiolus)
• Divided by the basilar membrane (below — scala tympani) and Reissner's membrane (above — scala vestibuli)
• The space between = scala media (cochlear duct) — the membranous labyrinth portion; contains the organ of Corti (receptor cells for hearing) on the basilar membrane
• High frequencies detected at the base; low frequencies at the apex (tonotopic mapping)
2. Vestibule (central part):
• Contains the oval window (stapes footplate) and round window
• Communicates with the semicircular canals posteriorly and the cochlea anteriorly
• Contains the utricle and saccule (membranous labyrinth portions for linear acceleration and gravity)
3. Semicircular canals (for rotational equilibrium):
• Three canals: anterior (superior), posterior, lateral (horizontal)
• Each has an ampulla at one end containing the crista ampullaris (receptor for angular acceleration)
• The three canals are oriented at 90° to each other — allowing detection of rotation in any plane
Membranous Labyrinth Summary:
• Cochlear duct (scala media) → hearing via organ of Corti (CN VIII cochlear branch)
• Utricle and saccule → linear acceleration/gravity via macula (CN VIII vestibular branch)
• Semicircular ducts → angular acceleration via crista ampullaris (CN VIII vestibular branch)
The vestibulocochlear nerve (CN VIII) transmits all signals from the internal ear to the brainstem via the internal auditory meatus.
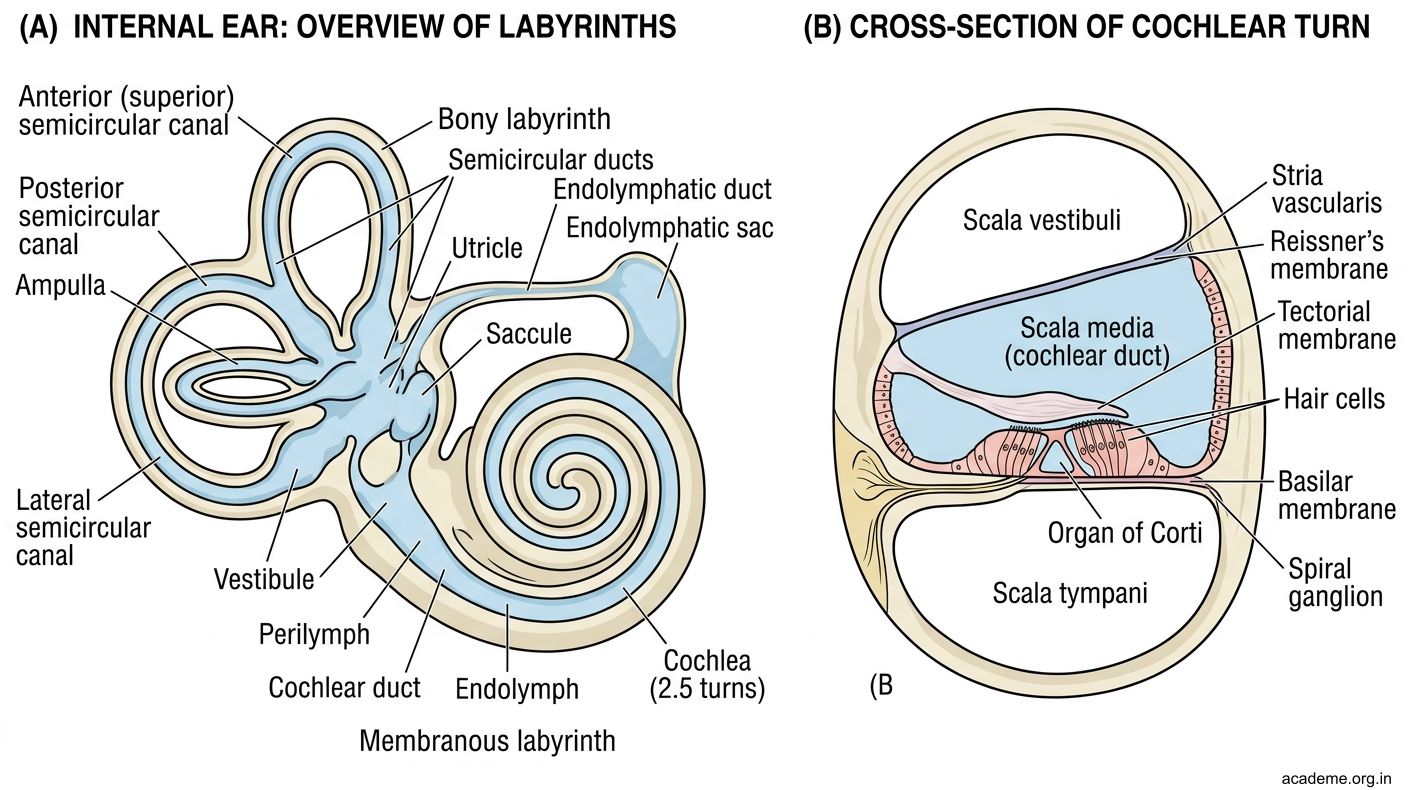
Figure: Part 3: Internal Ear (AN40.3)

Figure: Bony Labyrinth — Three parts:

Figure: Bony Labyrinth — Three parts:
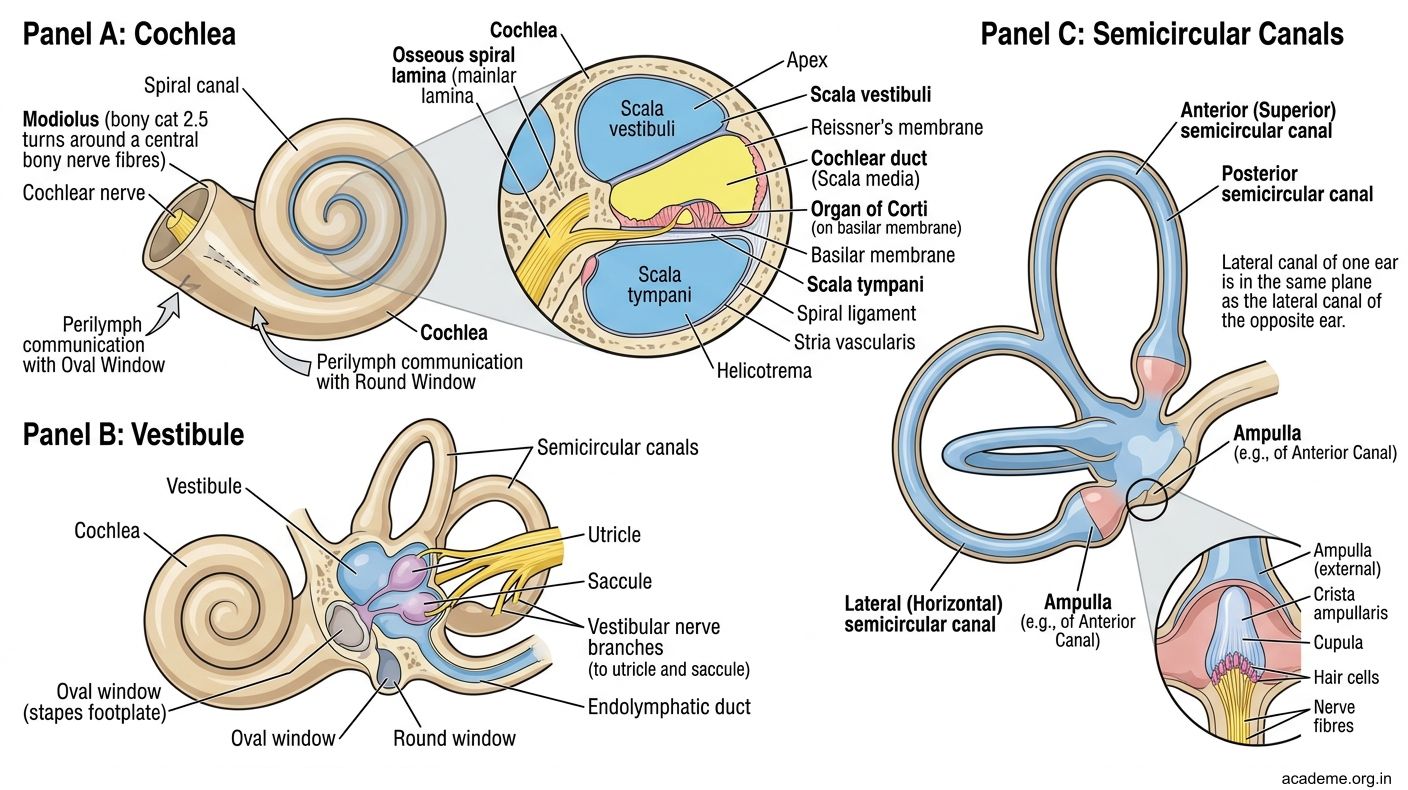
Figure: Bony Labyrinth — Three parts:
Part 4: Otitis Media, Otitis Externa, and Myringotomy (AN40.4–40.5)
Otitis Externa — Anatomical Basis (AN40.4)

Figure: Key Takeaways — Organs of Hearing and Equilibrium (AN40.1-5)

Figure: Cholesteatoma — The Dangerous Ear

Figure: Myringotomy — Anatomical Basis (AN40.5)

Figure: Otitis Media — Anatomical Complications (AN40.4)

Figure: Part 4: Otitis Media, Otitis Externa, and Myringotomy (AN40.4–40.5)
Otitis externa = inflammation/infection of the external auditory meatus.
Why it occurs:
• The cartilaginous EAM contains hair follicles and ceruminous glands — potential entry points for bacteria (Pseudomonas, Staphylococcus)
• Swimmer's ear — prolonged water exposure changes EAM pH and removes protective cerumen
• Diabetes — impaired immunity + malignant (necrotising) otitis externa caused by Pseudomonas aeruginosa — can spread to skull base causing osteomyelitis
Key anatomical relationships:
• The parotid gland lies anterior to the cartilaginous EAM (explaining referred pain to the parotid region)
• Fissures of Santorini — gaps in the cartilaginous wall of the anterior EAM — allow infection to spread to the parotid gland
• In malignant otitis externa, infection can spread posteriorly to the stylomastoid foramen — causing facial nerve palsy
Otitis Media — Anatomical Complications (AN40.4)
Infection in the middle ear can spread to adjacent structures because of the relationships of the tympanic cavity walls:
| Direction of spread | Structure involved | Complication |
|---|---|---|
| Superiorly (through tegmen tympani) | Middle cranial fossa → brain | Extradural abscess, meningitis, temporal lobe abscess |
| Posteriorly (through aditus) | Mastoid antrum → mastoid air cells | Acute/chronic mastoiditis |
| Laterally | Tympanic membrane | Perforation (protective — relieves pressure) |
| Medially | Labyrinthine wall → inner ear | Labyrinthitis (hearing loss + vertigo) |
| Inferiorly | Jugular bulb | Sigmoid sinus thrombosis |
| Along facial nerve canal | CN VII horizontal portion | Facial nerve palsy |
Myringotomy — Anatomical Basis (AN40.5)
Myringotomy = surgical incision through the tympanic membrane to drain middle ear fluid/pus.
Why the anteroinferior quadrant?
The tympanic membrane is divided into four quadrants by two lines:
• Vertical line through the handle of malleus
• Horizontal line through the umbo
The anteroinferior quadrant is chosen because:
• It is farthest from the ossicles (malleus handle is anterior-superior)
• It is farthest from the facial nerve (which crosses the posterior-superior quadrant)
• It avoids the chorda tympani (runs in the posterior-superior region between malleus and incus)
• It avoids the round window (postero-inferior)
Structures to avoid:
• Posterosuperior quadrant — most dangerous; contains the chorda tympani, ossicles, facial nerve canal, and proximity to the lateral semicircular canal
• Posteroinferior — close to the round window
After myringotomy, a grommet (ventilation tube) is inserted to maintain drainage and pressure equalisation in recurrent otitis media with effusion ("glue ear").
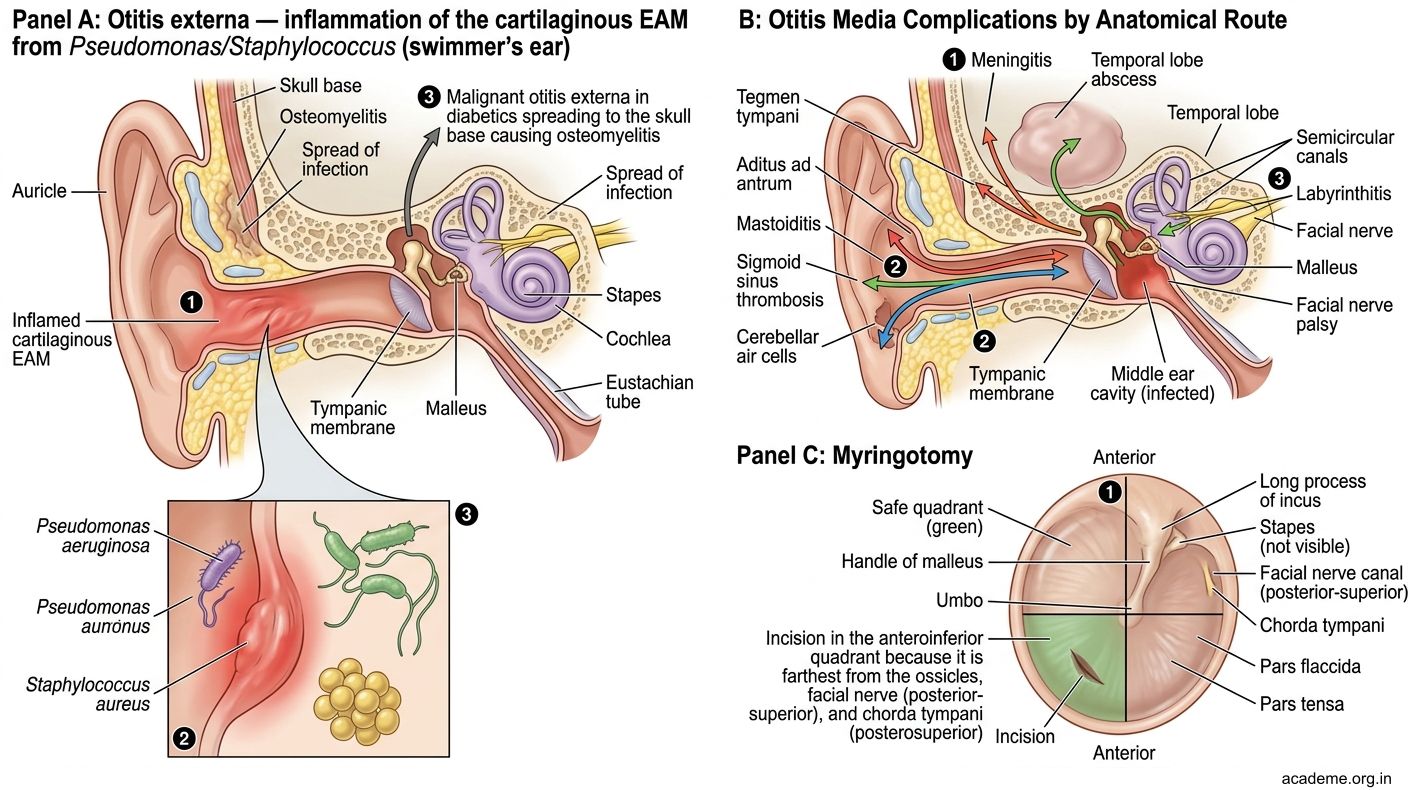
Figure: Part 4: Otitis Media, Otitis Externa, and Myringotomy (AN40.4–40.5)
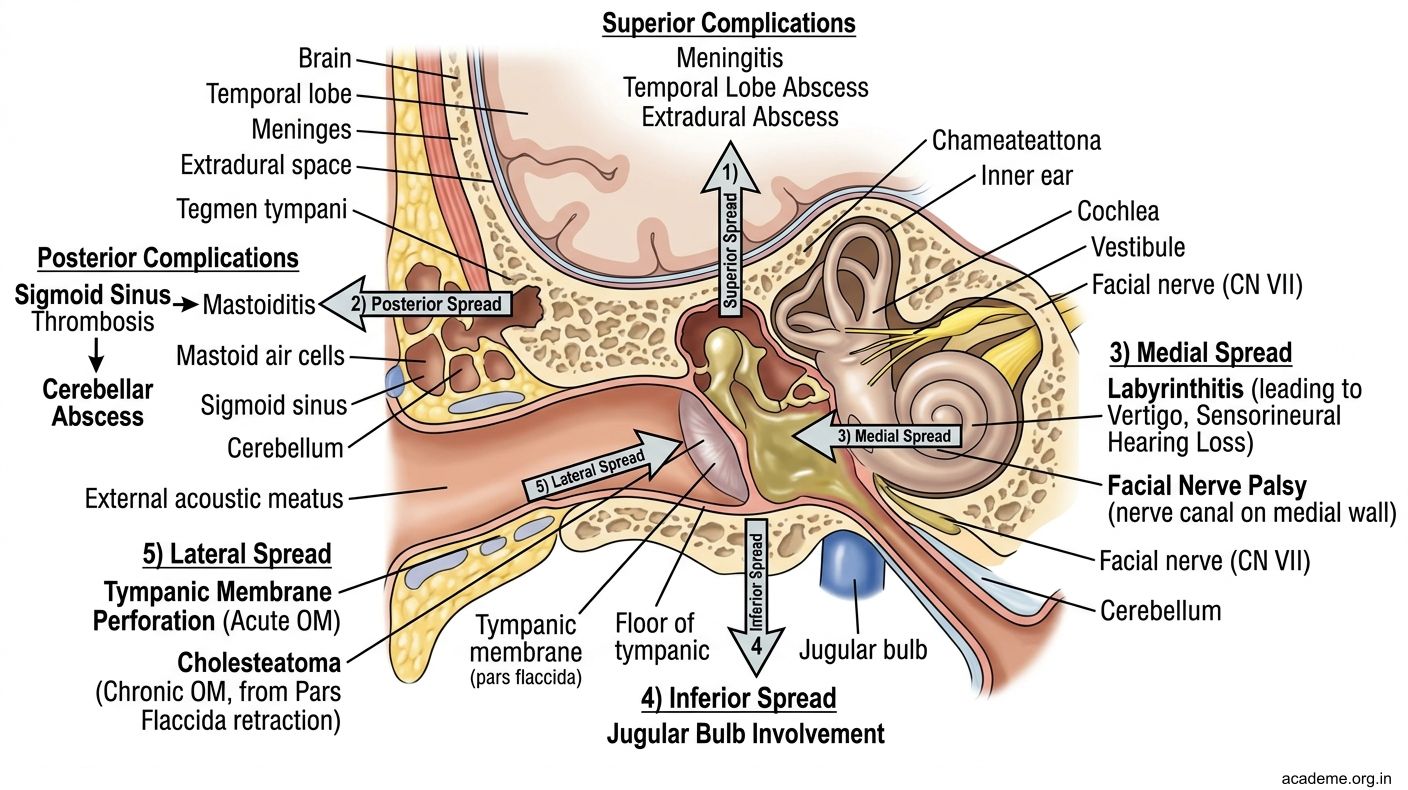
Figure: Otitis Media — Anatomical Complications (AN40.4)
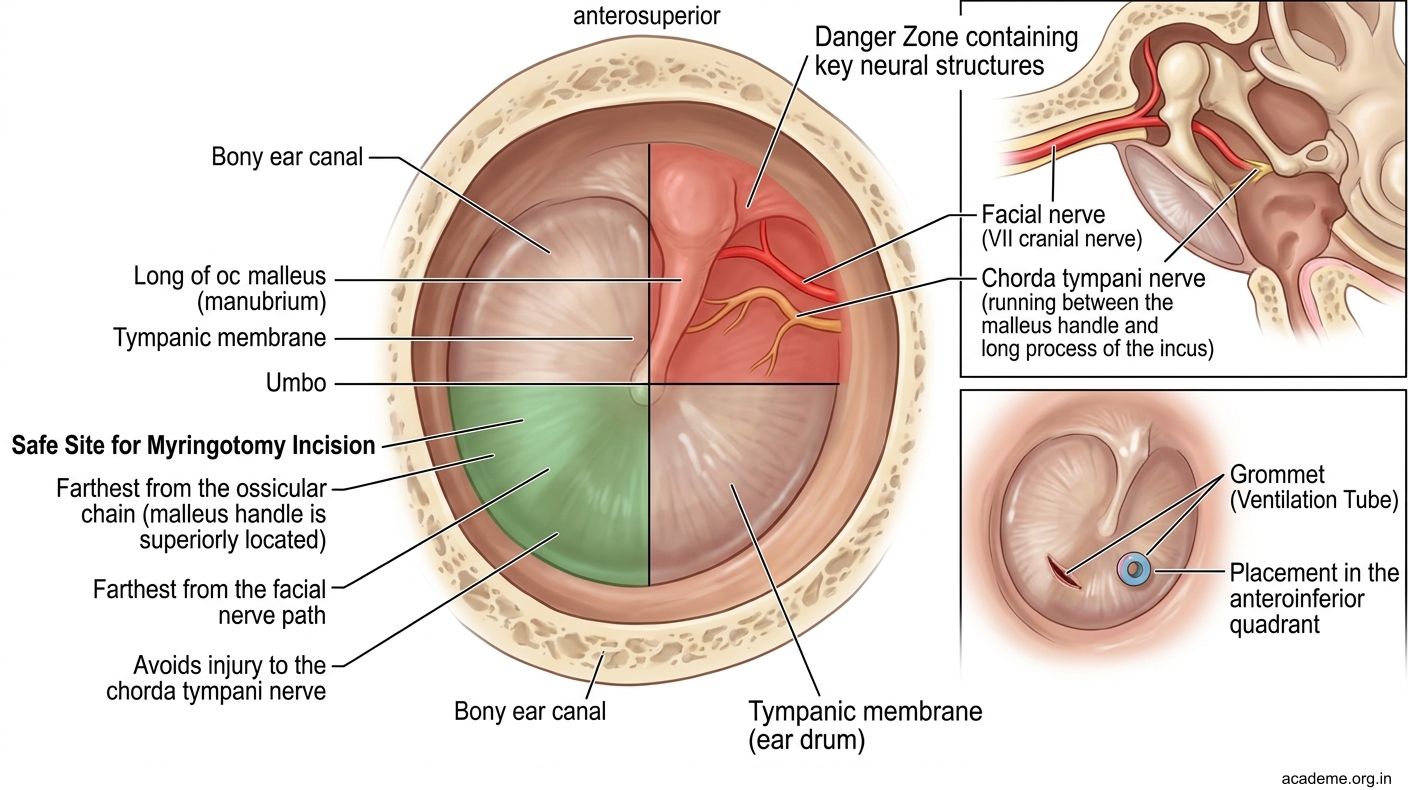
Figure: Myringotomy — Anatomical Basis (AN40.5)
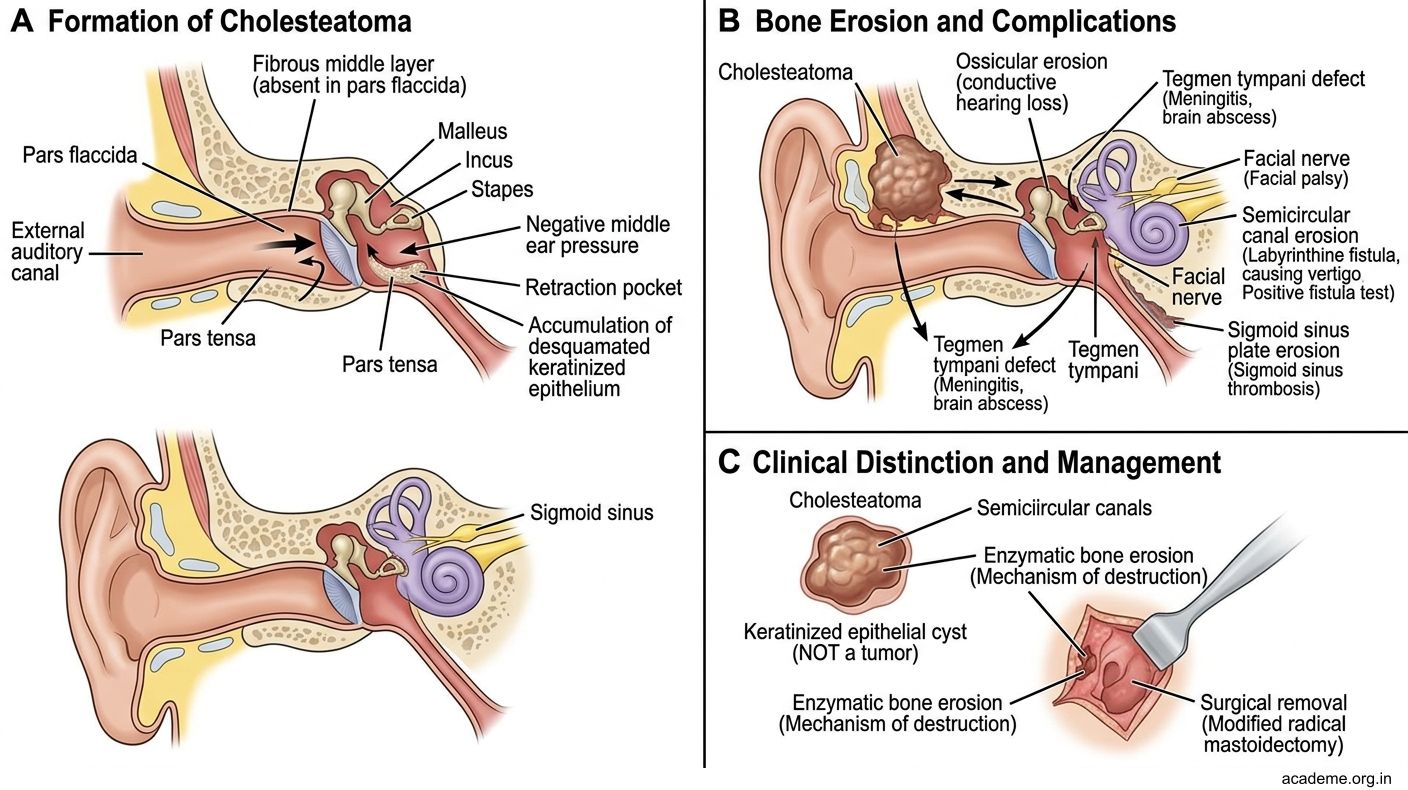
Figure: Cholesteatoma — The Dangerous Ear
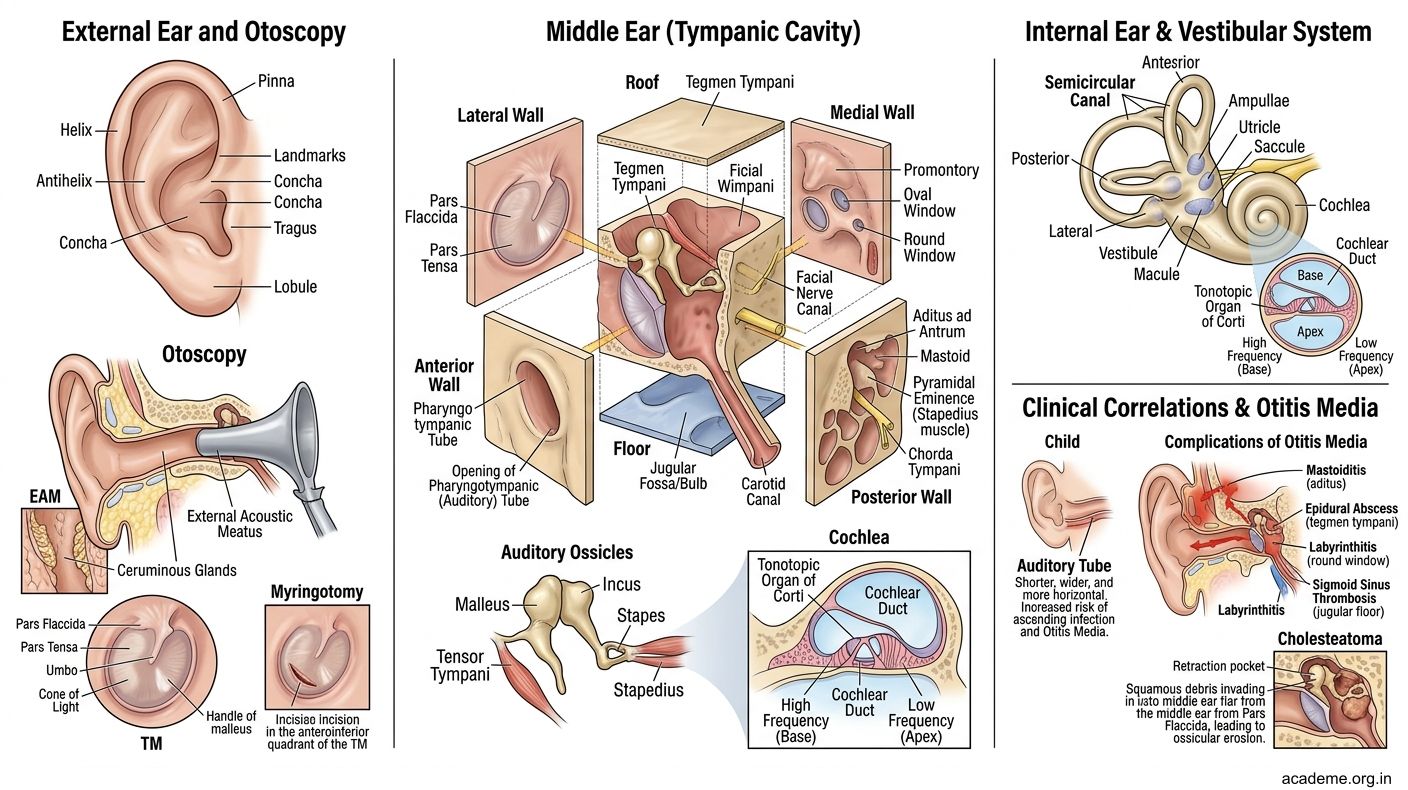
Figure: Key Takeaways — Organs of Hearing and Equilibrium (AN40.1-5)
SELF-CHECK — : Internal Ear and Clinical Applications
A patient with chronic otitis media develops sudden facial nerve palsy and vertigo. Which wall of the middle ear has the infection most likely eroded?
A. Lateral (tympanic) wall
B. Medial (labyrinthine) wall
C. Anterior (carotid) wall
D. Floor (jugular) wall
Reveal Answer
Answer: B. Medial (labyrinthine) wall
During myringotomy, the incision is made in the anteroinferior quadrant primarily to avoid:
A. The tympanic plexus on the promontory
B. The chorda tympani and facial nerve in the posterosuperior region
C. The internal carotid artery on the anterior wall
D. The opening of the auditory tube
Reveal Answer
Answer: B. The chorda tympani and facial nerve in the posterosuperior region
The high-pitched (high-frequency) sounds are detected at which part of the cochlea?
A. Apex (helicotrema)
B. Modiolus
C. Base (near oval window)
D. Scala vestibuli at mid-turn
Reveal Answer
Answer: C. Base (near oval window)
CLINICAL PEARL
Cholesteatoma — The Dangerous Ear
A cholesteatoma is a cyst-like accumulation of keratinising squamous epithelium in the middle ear or mastoid. It arises from the pars flaccida (Shrapnell's membrane) — the flaccid, unsupported upper part of the tympanic membrane.
The pars flaccida lacks the fibrous middle layer of the pars tensa. Negative pressure in the middle ear (from Eustachian tube dysfunction) sucks the pars flaccida inward, forming a retraction pocket that fills with desquamated epithelium.
As the cholesteatoma enlarges, it produces collagenases that erode bone — destroying the ossicles (causing conductive hearing loss), breaching the tegmen tympani (causing meningitis or brain abscess), eroding the facial nerve canal (causing facial palsy), or invading the labyrinth (causing sensorineural hearing loss and vertigo).
Clinical cue: Foul-smelling, painless, unilateral ear discharge in a child or adult — suspect cholesteatoma until proven otherwise. Otoscopy shows a white mass in the attic region (above the pars tensa). Requires CT temporal bone and surgical excision (mastoidectomy).
REFLECT
Return to the hook case — the 9-year-old with acute otitis media and tympanic membrane perforation.
- Via which anatomical route did the infection most likely travel from the nasopharynx to the middle ear?
- The doctor decided to perform myringotomy. In which quadrant should the incision be made, and why?
- If the infection had NOT ruptured the membrane and had instead spread superiorly, what would be the most dreaded complication?
- If this child had recurrent attacks of otitis media, what anatomical factor in children predisposes them, and what non-surgical and surgical interventions address this?
Discussion: Infection travels via the auditory (Eustachian) tube from the nasopharynx. The tube in a 9-year-old is still relatively short and horizontal. Myringotomy should be in the anteroinferior quadrant to avoid the facial nerve, chorda tympani, and ossicles in the posterosuperior quadrant. Superior spread through the tegmen tympani into the middle cranial fossa would cause extradural abscess or meningitis. Recurrent infections → consider adenoidectomy (to reduce nasopharyngeal bacterial load) + grommet insertion for chronic otitis media with effusion.
KEY TAKEAWAYS
Key Takeaways — Organs of Hearing and Equilibrium (AN40.1-5)
External Ear:
• EAM: outer 1/3 cartilaginous (wax glands + hair), inner 2/3 bony
• Nerve supply: CN V3 (auriculotemporal) anteriorly, CN X (Arnold's nerve) posteriorly, C2,C3 (great auricular) posterior auricle
• Otoscopy in adults: pull pinna upward+backward; children: downward+backward
Middle Ear (6 walls):
• Lateral = tympanic membrane (pars tensa + pars flaccida)
• Medial = oval window + round window + promontory + facial nerve canal
• Anterior = auditory tube opening + carotid wall
• Posterior = aditus to mastoid
• Roof = tegmen tympani (dura above), Floor = jugular bulb below
• Ossicles: malleus-incus-stapes; tensor tympani (CN V3) + stapedius (CN VII)
Auditory Tube: shorter + horizontal in children → higher otitis media risk
Internal Ear:
• Cochlea → hearing (organ of Corti, CN VIII cochlear)
• Utricle/saccule → linear acceleration (macula, CN VIII vestibular)
• Semicircular canals → angular acceleration (crista ampullaris)
• Filled with endolymph (high K⁺); perilymph in surrounding bony labyrinth
Myringotomy: anteroinferior quadrant — safest; avoids CN VII, chorda tympani, ossicles
Complications of otitis media: mastoiditis (posterior), meningitis/abscess (superior through tegmen), labyrinthitis (medial), facial palsy (facial nerve canal), sigmoid sinus thrombosis (inferior)