Page 3 of 12
MI1.10 | Staining Techniques — Gram & ZN (Practical) — SDL Guide
Learning Objectives
- Describe the principle and rationale of the Gram staining technique
- Perform the Gram stain procedure step-by-step on a clinical specimen smear
- Interpret Gram stain results to identify organisms by morphology, arrangement, and Gram reaction
- Describe the principle of the Ziehl-Neelsen (ZN) acid-fast staining technique
- Perform and interpret ZN staining on a sputum smear for mycobacteria
- Describe the principle and procedure for routine stool examination for identification of parasitic agents
INSTRUCTIONS
This is a procedure-focused module. Accurate staining technique and confident interpretation are core practical competencies in MBBS and remain essential clinical skills: Gram stain interpretation guides immediate empiric antibiotic decisions; ZN smear interpretation is the first-line diagnostic for pulmonary tuberculosis. Use the IMAGE markers to visualise what you should see at each step and under the microscope.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, 11th ed., Ch 3 & Practical Manual (textbook)
- Mackie & McCartney Practical Medical Microbiology, 14th ed., Ch 5 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2 AM. A 65-year-old diabetic man is brought in obtunded with fever and a purulent sputum. Blood cultures have been sent but results will take 48 hours. The single test that will guide your immediate antibiotic choice is the Gram stain of his sputum, which you can have in 15 minutes. You see Gram-positive diplococci in pairs. Streptococcus pneumoniae — you start benzyl penicillin. This 120-year-old technique remains your fastest diagnostic tool.
WHY THIS MATTERS
Gram stain identifies organisms within 15-20 minutes of receiving a specimen — it guides empiric antibiotic therapy before culture results are available. ZN smear is the primary diagnostic test for pulmonary TB in India, where TB remains a major public health burden; smear microscopy is the initial test for over 1.5 million people annually under NTEP. Routine stool examination identifies intestinal parasites — a leading cause of malnutrition and anaemia in children in endemic regions. These are not academic exercises — they are daily tools of clinical microbiology.
RECALL
Recall from the Microbiology introduction module that Gram-positive bacteria have a thick peptidoglycan cell wall (20-80 nm) and Gram-negative bacteria have a thin peptidoglycan (2-7 nm) with an additional outer membrane. Also recall that Mycobacteria have a unique, highly lipid-rich (mycolic acid-containing) cell wall that makes them resistant to conventional staining but, once stained, also resistant to acid decolourisation — the basis of 'acid-fastness'.
Gram Staining — Principle
Principle of Gram Staining
The Gram stain differentiates bacteria into two broad groups based on cell wall architecture.
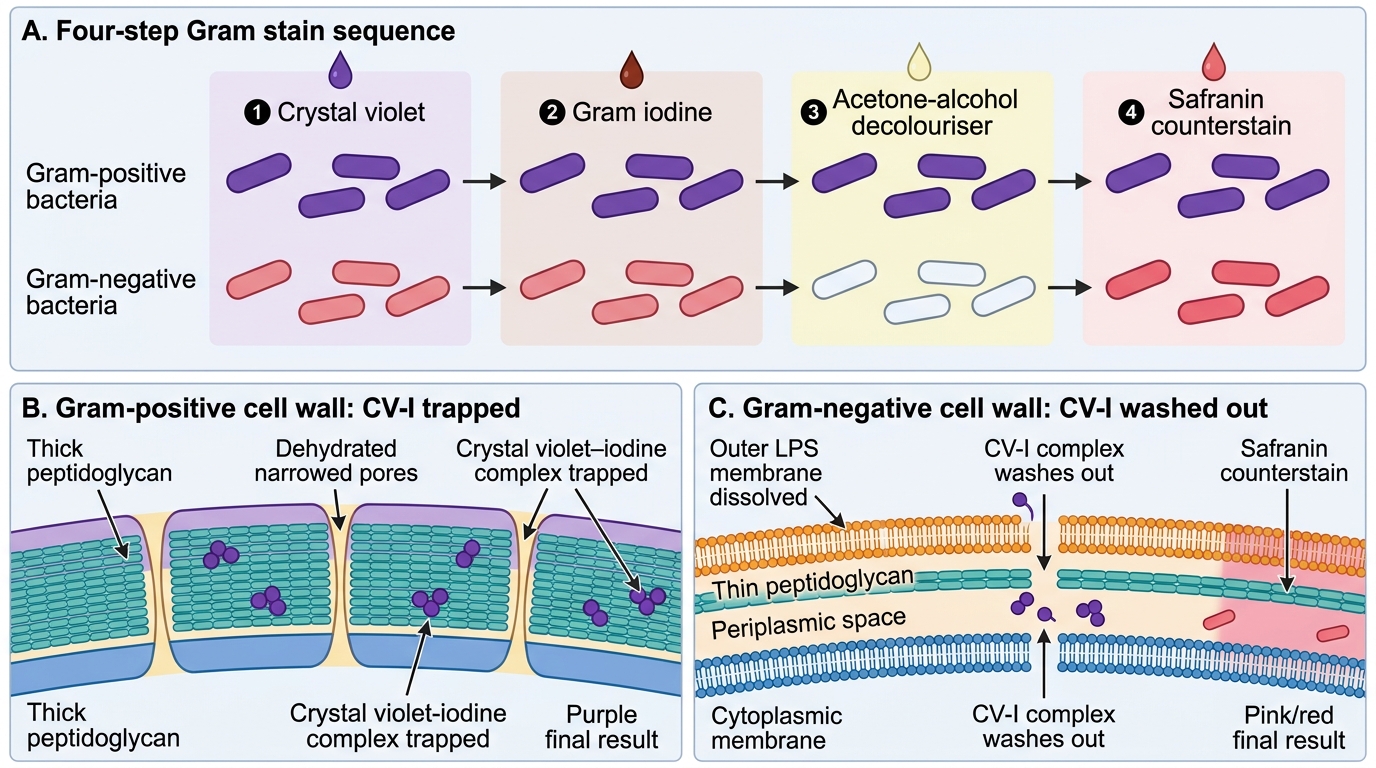
Mechanism — why Gram-positive bacteria retain crystal violet:
1. Crystal violet (primary stain) + Gram's iodine (mordant) form an insoluble crystal violet-iodine (CV-I) complex within the cell.
2. Decolouriser (acetone-alcohol) — removes lipids and dehydrates the thick peptidoglycan in Gram-positive organisms, which then contracts and traps the CV-I complex → cell remains purple.
3. In Gram-negative organisms, the decolouriser dissolves the outer lipopolysaccharide membrane, creating channels through the thin peptidoglycan layer → CV-I complex washes out → cell appears colourless.
4. Safranin (counterstain) — stains decolourised Gram-negative organisms pink/red.
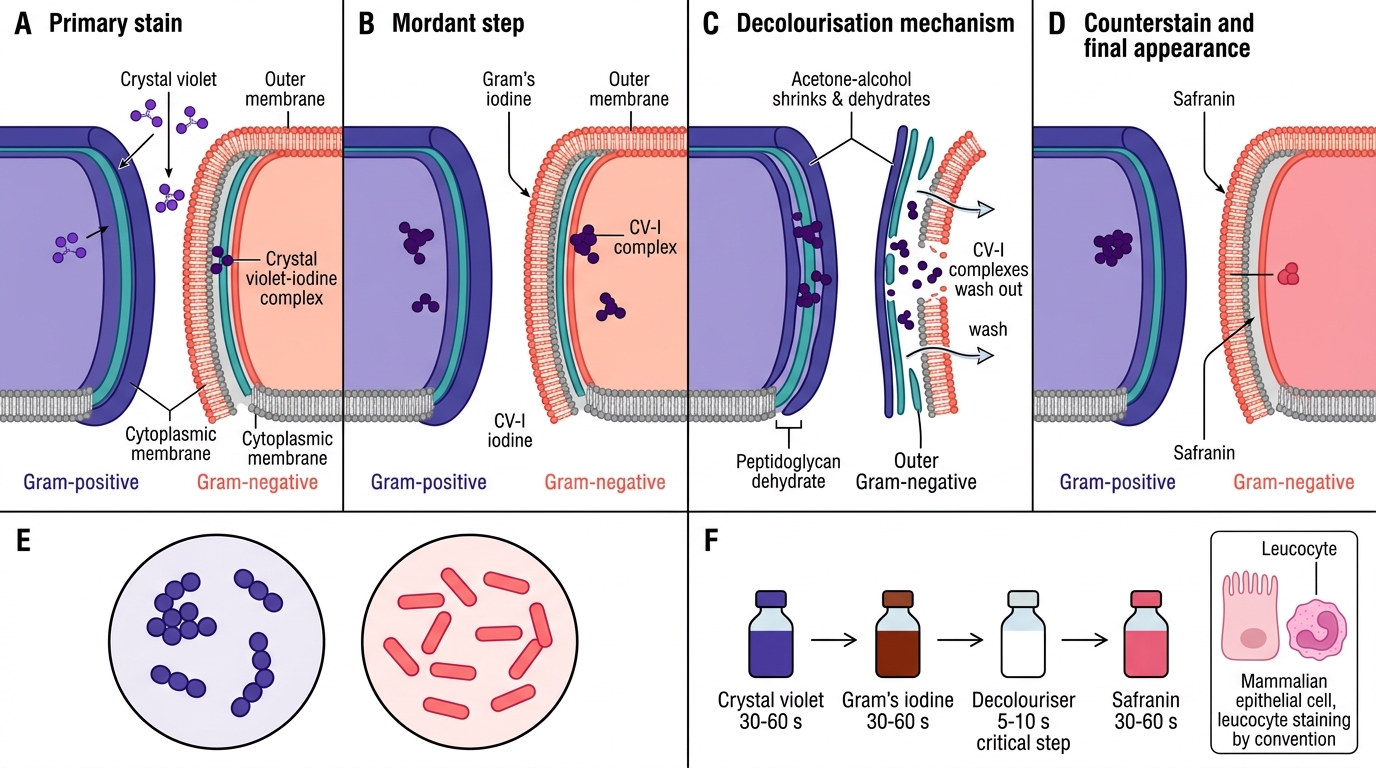
Gram Stain Mechanism: CV-I Retention versus Wash-Out
Result:
• Gram-positive → purple/violet
• Gram-negative → pink/red
• Mammalian cells (epithelial, leucocytes) → pink (Gram-negative by convention)
Gram Staining — Procedure
Gram Staining Procedure
Materials required: glass slides, heat-fixed smear, crystal violet, Gram's iodine, acetone-alcohol (decolouriser), safranin, wash bottle with water, staining rack, blotting paper.
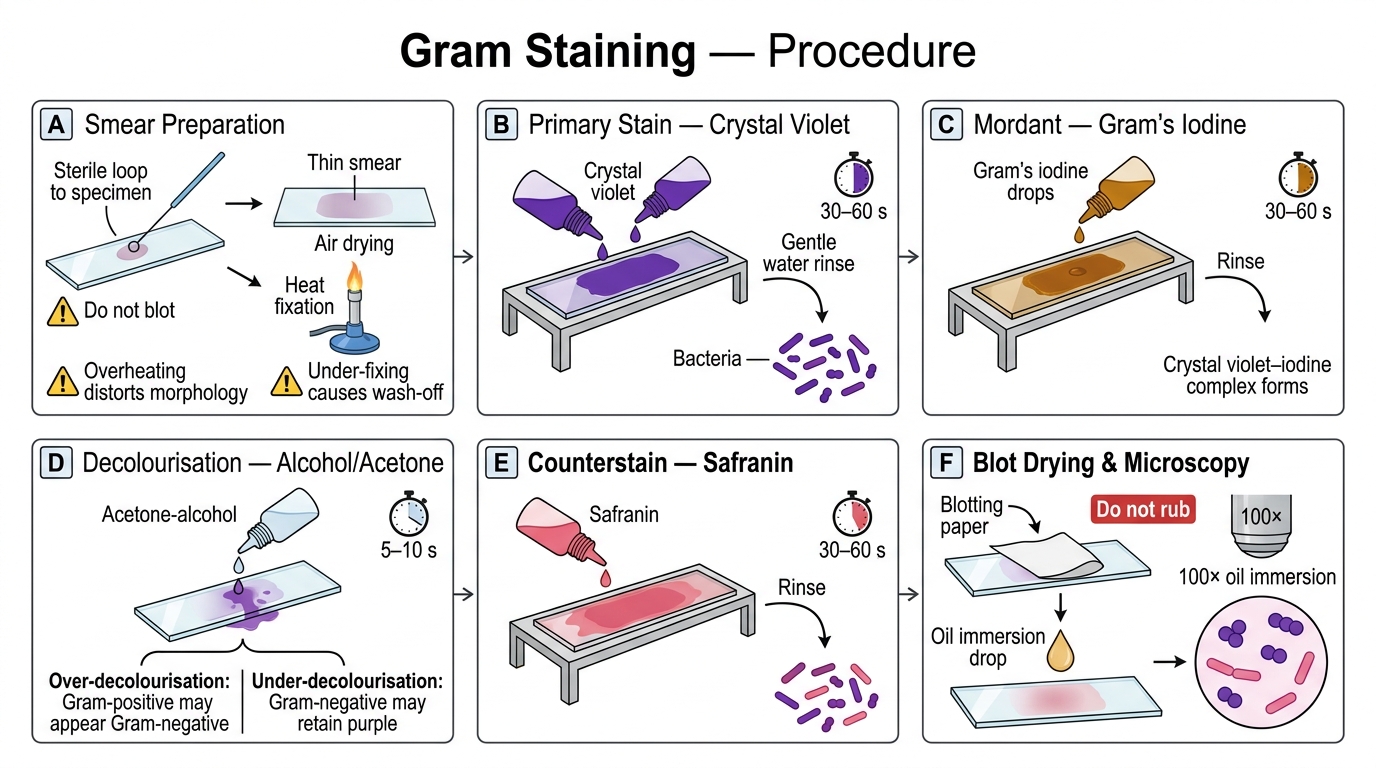
Step-by-step procedure:
1. Smear preparation:
• Clean a glass slide (degrease with alcohol).
• Using a sterile loop or swab, prepare a thin smear of the specimen on the slide.
• Allow to air-dry completely (do not blot).
• Heat-fix: pass slide quickly 2-3 times through a Bunsen flame (underside of slide). Heat-fixing kills organisms and adheres them to the slide. Over-heating distorts morphology; under-fixing causes wash-off.
2. Crystal violet (primary stain): flood the smear, wait 30-60 seconds, rinse with water gently.
3. Gram's iodine (mordant): flood the smear, wait 30-60 seconds, rinse with water gently.
4. Decolouriser (acetone-alcohol): apply drop-by-drop until no more purple colour washes off — typically 5-10 seconds. This is the most critical step: over-decolourisation converts Gram-positives to apparent Gram-negatives; under-decolourisation falsely retains colour in Gram-negatives.
5. Safranin (counterstain): flood, wait 30-60 seconds, rinse with water.
6. Blot dry gently. Do NOT rub.
7. Microscopy: examine under oil immersion (×100 objective, ×10 eyepiece = ×1000 total magnification).

Correct Gram Stain in a Mixed Specimen
Common technical errors:
• Over-decolourisation → false Gram-negative result (most common error)
• Under-decolourisation → false Gram-positive result
• Smear too thick → morphology obscured
• Heat-fixing too hot → shrunken, distorted cells
• Safranin applied before complete decolourisation → background staining
Gram Stain Interpretation
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Gram Stain Interpretation
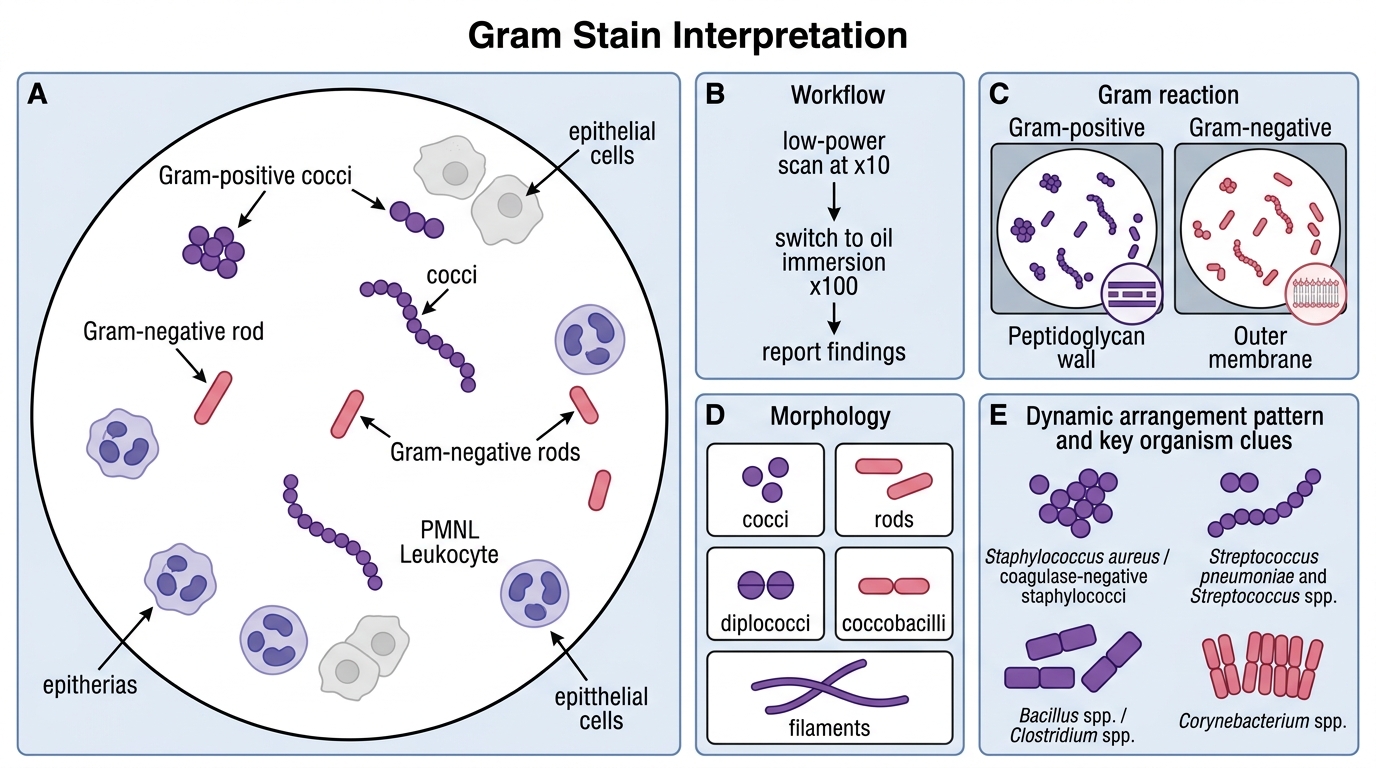
Systematic reading of every Gram stain:
Step 1 — Scan at low power (×10) to identify areas where cells are sparse and well-separated (avoid thick clumps).
Step 2 — Switch to oil immersion (×100) for identification.
Step 3 — Report:
• Gram reaction (positive/negative)
• Morphology (cocci, rods, diplococci, coccobacilli, filaments)
• Arrangement (singles, pairs, clusters, chains, palisades)
• Any other cells (pus cells — PMNLs, epithelial cells)
Key organisms by Gram stain appearance:
| Appearance | Organisms to consider |
|---|---|
| Gram+ cocci in clusters | Staphylococcus aureus, coagulase-negative staphylococci |
| Gram+ cocci in pairs/chains | Streptococcus pneumoniae (diplococci, lancet-shaped), Streptococcus spp. |
| Gram+ rods (large, boxcar-shaped) | Bacillus spp., Clostridium spp. |
| Gram+ rods (Chinese letter/palisade) | Corynebacterium spp. |
| Gram− diplococci (kidney-shaped, intracellular in PMNLs) | Neisseria gonorrhoeae, N. meningitidis |
| Gram− rods (straight) | Enterobacteriaceae (E. coli, Klebsiella, Salmonella) |
| Gram− coccobacilli | Haemophilus influenzae |
| Gram-variable/indeterminate | Mycobacteria (will not stain well — use ZN) |
Sputum quality assessment by Gram stain:
A valid sputum sample should show >25 PMNLs and <10 squamous epithelial cells per low-power field. Samples with predominant squamous cells are mouth-wash samples (saliva) — reject and request a repeat deep cough specimen.

Key Gram Stain Appearances in Medical Microbiology
SELF-CHECK
You are performing a Gram stain on a urethral discharge. After completing the procedure, you observe kidney-shaped diplococci inside neutrophils (PMNLs) staining pink. What is the most likely interpretation?
A. Gram-positive diplococci — likely Streptococcus pneumoniae
B. Gram-negative diplococci — likely Neisseria gonorrhoeae
C. Gram-positive cocci in clusters — likely Staphylococcus aureus
D. Over-decolourised Gram-positive cocci — repeat stain
Reveal Answer
Answer: B. Gram-negative diplococci — likely Neisseria gonorrhoeae
Pink staining with safranin indicates Gram-negative organisms. Kidney-shaped (reniform) diplococci located intracellularly within neutrophils (PMNLs) in urethral discharge are pathognomonic of Neisseria gonorrhoeae. This finding in the correct clinical context (urethral discharge) has high sensitivity and specificity and warrants immediate treatment. Streptococcus pneumoniae diplococci are Gram-positive (purple) and lancet-shaped.