Page 2 of 12
MI1.12-13 | Sterilisation & Disinfection — SDL Guide
Learning Objectives
- Classify and describe physical and chemical methods of sterilisation and disinfection
- Explain the mechanism of action of each method
- Describe quality control measures for sterilisation methods used in laboratory and clinical settings
- Choose the most appropriate method of sterilisation or disinfection for a given material, setting, or clinical situation
- Differentiate sterilisation from disinfection, antisepsis, and decontamination using defined criteria
INSTRUCTIONS
Hospital-acquired infections (HAIs) cause an estimated 1.4 million preventable deaths globally each year. Proper sterilisation and disinfection practices are the primary defence. This module gives you the scientific basis, practical decision-making framework, and quality control tools you need to choose and apply these methods correctly in the clinic, theatre, and laboratory.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, 11th ed., Ch 3 (textbook)
- Mandell, Douglas & Bennett's Principles of Infectious Diseases, 9th ed., Ch 15 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In 2015, a cluster of carbapenem-resistant Klebsiella pneumoniae infections occurred at a US hospital following endoscopic retrograde cholangiopancreatography (ERCP). Investigation revealed that the duodenoscopes — reusable instruments with complex elevator mechanisms — were not being adequately disinfected between patients. The elevator channel harboured biofilm-protected bacteria despite the recommended high-level disinfection protocol. This outbreak, which killed several patients, ultimately triggered a complete redesign of duodenoscope reprocessing protocols. The science of sterilisation is not an administrative formality — it is life-critical engineering.
WHY THIS MATTERS
As a clinician you will order procedures that require sterile instruments daily — IV cannulation, lumbar puncture, surgery, wound dressing. You must be able to: judge whether an instrument has been properly sterilised; select the correct disinfectant for a contaminated surface; counsel a patient on antisepsis of a wound at home; and recognise when a sterilisation failure may have occurred. These are active clinical responsibilities, not just policies for the sterile services department.
RECALL
From Year-1 Biochemistry, recall that proteins are denatured by heat (breaking non-covalent bonds), strong acids/bases (disrupting charge interactions), and certain solvents (disrupting hydrophobic cores). From your Microbiology introduction, recall that bacterial endospores are metabolically dormant and highly resistant. Also remember that bacterial cell walls contain peptidoglycan and that Gram-negative bacteria have an additional outer membrane — both relevant to why different agents have different spectra of activity.
Key Definitions
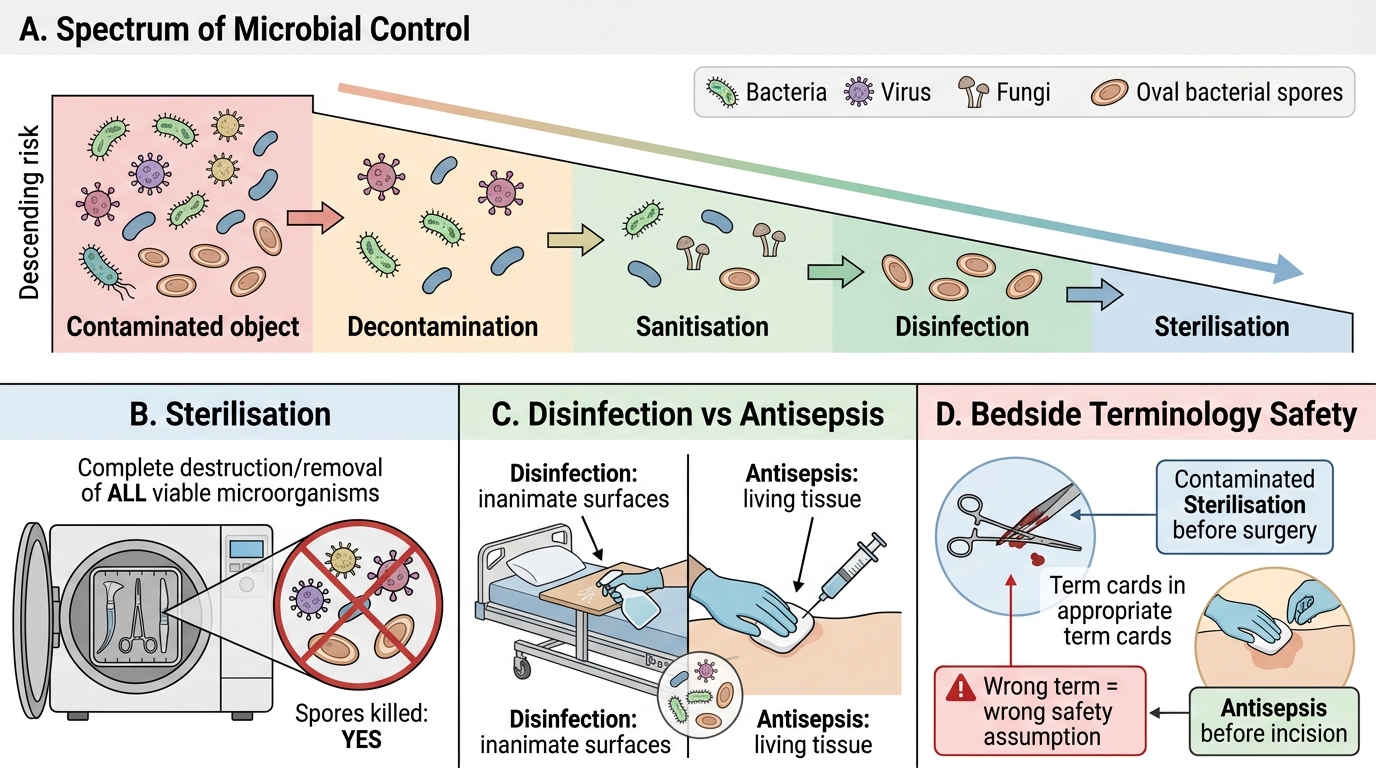
Key Definitions in Microbial Control
Precise terminology prevents dangerous errors at the bedside and in the operating theatre:
| Term | Definition | Kills spores? |
|---|---|---|
| Sterilisation | Complete destruction or removal of ALL viable microorganisms, including spores | Yes |
| Disinfection | Elimination of most pathogenic organisms from inanimate surfaces; may not eliminate spores or all viruses | No (generally) |
| Antisepsis | Disinfection applied to living tissue (skin, mucous membranes) | No |
| Decontamination | Reduction of microbial load on an object/surface to a safe level | No |
| Sanitisation | Reduction of microbial load to levels deemed safe by public health standards | No |
| Bacteriostatic | Inhibits bacterial growth without killing | No |
| Bactericidal | Kills bacteria | Depends on agent |
| Sporicidal | Kills bacterial spores | Yes |
Spaulding classification — guides instrument processing choice:
• Critical items (penetrate sterile tissue or vasculature): must be sterilised — surgical instruments, needles, implants
• Semi-critical items (contact mucous membranes): minimum high-level disinfection — endoscopes, laryngoscope blades, respiratory therapy equipment
• Non-critical items (contact intact skin only): low/intermediate-level disinfection — blood pressure cuffs, stethoscopes, bedpans
Physical Methods of Sterilisation
Physical Methods of Sterilisation by Heat
Heat — the most reliable and widely used method
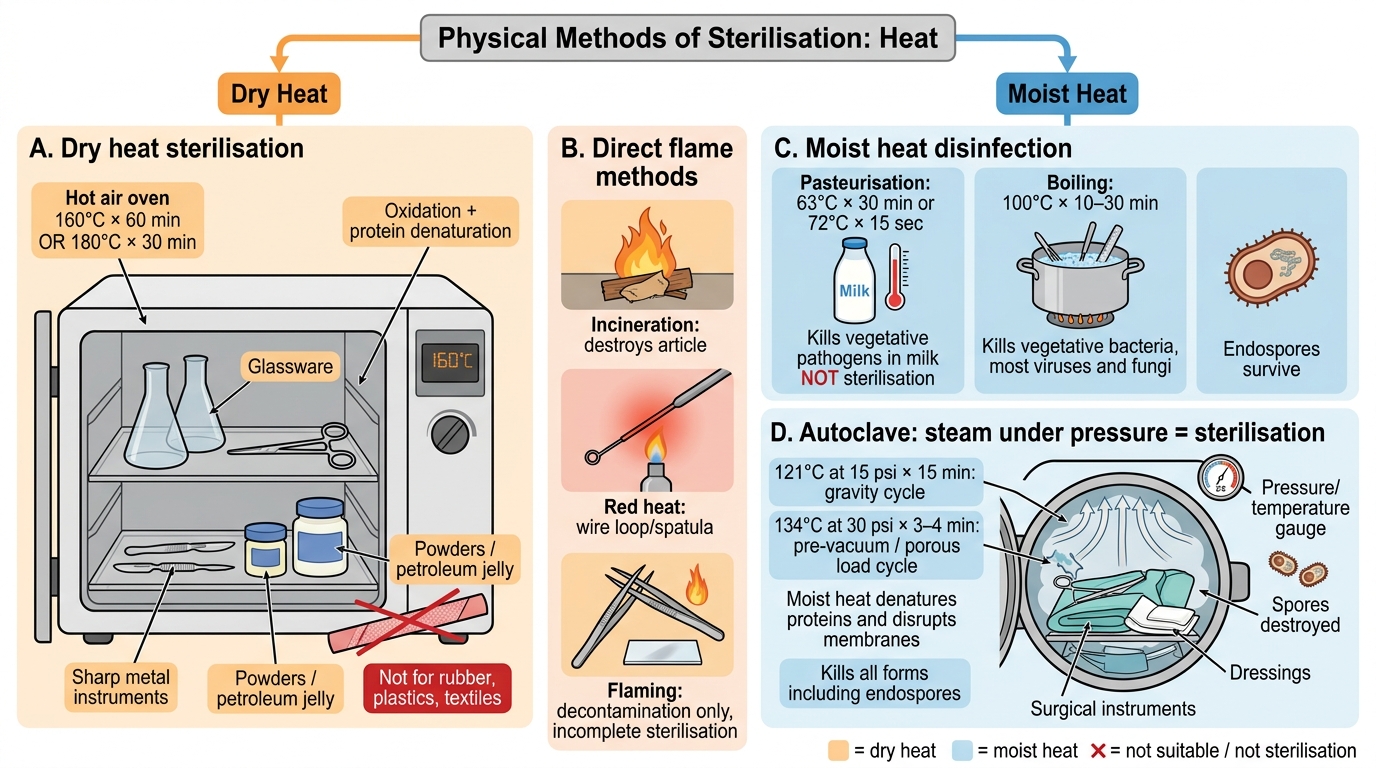
Dry heat:
• Hot air oven: 160°C × 60 min, or 180°C × 30 min. Mechanism: oxidation, protein denaturation. Used for glassware, metal instruments with sharp edges (scalpels, scissors), petroleum jelly, powders. NOT for rubber, plastics, textiles.
• Incineration: direct burning — for infectious waste, contaminated material, disposable items. Rapid but destroys the article.
• Red heat: flaming wire loops and spatulas in a Bunsen flame until red-hot — routine bacteriology bench technique.
• Flaming: rapid passage of metal forceps, slides through flame — incomplete sterilisation, used for decontamination only.
Moist heat (more efficient — water has greater thermal conductivity than dry air):
• Pasteurisation: 63°C × 30 min (holder/batch method) or 72°C × 15 sec (HTST); kills vegetative pathogens in milk (Mycobacterium bovis, Salmonella, Brucella) — NOT sterilisation.
• Boiling (100°C × 10-30 min): kills vegetative bacteria, most viruses and fungi. Does NOT kill endospores. Used for surgical instruments in resource-limited settings — equivalent to disinfection only.
• Autoclave (steam under pressure — sterilisation):
- 121°C at 15 psi × 15 min (gravity cycle — standard)
- 134°C at 30 psi × 3-4 min (pre-vacuum/porous load cycle — faster, better penetration)
- Mechanism: moist heat denatures proteins, disrupts membranes; kills all forms including endospores
- Used for: surgical instruments, dressings, culture media, laboratory glassware, waste
- Cannot be used for: heat-labile items (plastics, rubber, certain optics), oily preparations, sealed containers

Autoclave Cross-Section and Quality Control
### Quality control of autoclave
• Physical indicators: thermometer and pressure gauge readings recorded for every cycle
• Chemical indicators (Bowie-Dick test tape, TST strips): colour-change strips placed inside loads; verify temperature reached but NOT sterility
• Biological indicators (gold standard): paper strips or vials containing Geobacillus stearothermophilus spores (ATCC 7953) — most heat-resistant organism; incubated post-cycle, no growth confirms sterilisation
### Radiation
• Ionising radiation (gamma rays, electron beam): used commercially to sterilise single-use medical devices (syringes, catheters, gloves). Damages DNA by free radical formation. Cold sterilisation — no heat required. Not practical for hospital routine.
• Non-ionising radiation (UV, 254 nm wavelength): causes thymine dimer formation in DNA. Used to decontaminate laminar flow cabinets, OT air surfaces. Poor penetration — only line-of-sight; does not sterilise.
### Filtration
• Removes microorganisms by physical size exclusion; does NOT kill them.
• Membrane filters (0.22 µm): sterilise heat-labile liquids — serum, antibiotics, sugars, vitamin solutions. Does not remove viruses or prions.
• HEPA filters (High-Efficiency Particulate Air): remove 99.97% of particles ≥0.3 µm; used in laminar flow cabinets, operating theatres, isolation rooms.
CLINICAL PEARL
The autoclave is the workhorse of hospital sterilisation, but it fails silently when overloaded, improperly packed, or when items are not adequately pre-cleaned. The most common cause of autoclave sterilisation failure is organic matter (blood, pus, protein) creating a physical barrier that insulates organisms from steam penetration. This is why cleaning always precedes sterilisation — enzymatic detergents remove bioburden before autoclaving. In the OT, instruments must be cleaned, inspected, packaged, autoclaved, and QC-verified before use — each step is a critical link.
SELF-CHECK
A hospital OT manager needs to sterilise arthroscopic instruments with delicate lenses that will be damaged by autoclaving at 121°C. Which method should be chosen?
A. Hot air oven at 180°C × 30 min
B. UV radiation in a closed cabinet
C. Low-temperature hydrogen peroxide gas plasma
D. Boiling at 100°C × 30 min
Reveal Answer
Answer: C. Low-temperature hydrogen peroxide gas plasma
Delicate heat-labile optical instruments require low-temperature sterilisation. Hydrogen peroxide gas plasma (e.g., Sterrad) achieves sterilisation at 50-55°C through oxidative free radical mechanisms. Hot air oven and autoclave damage optics; UV only decontaminates surfaces in line-of-sight; boiling does not sterilise (does not kill spores) and may damage optics.
Chemical Methods of Disinfection and Sterilisation
Chemical Methods of Disinfection and Sterilisation
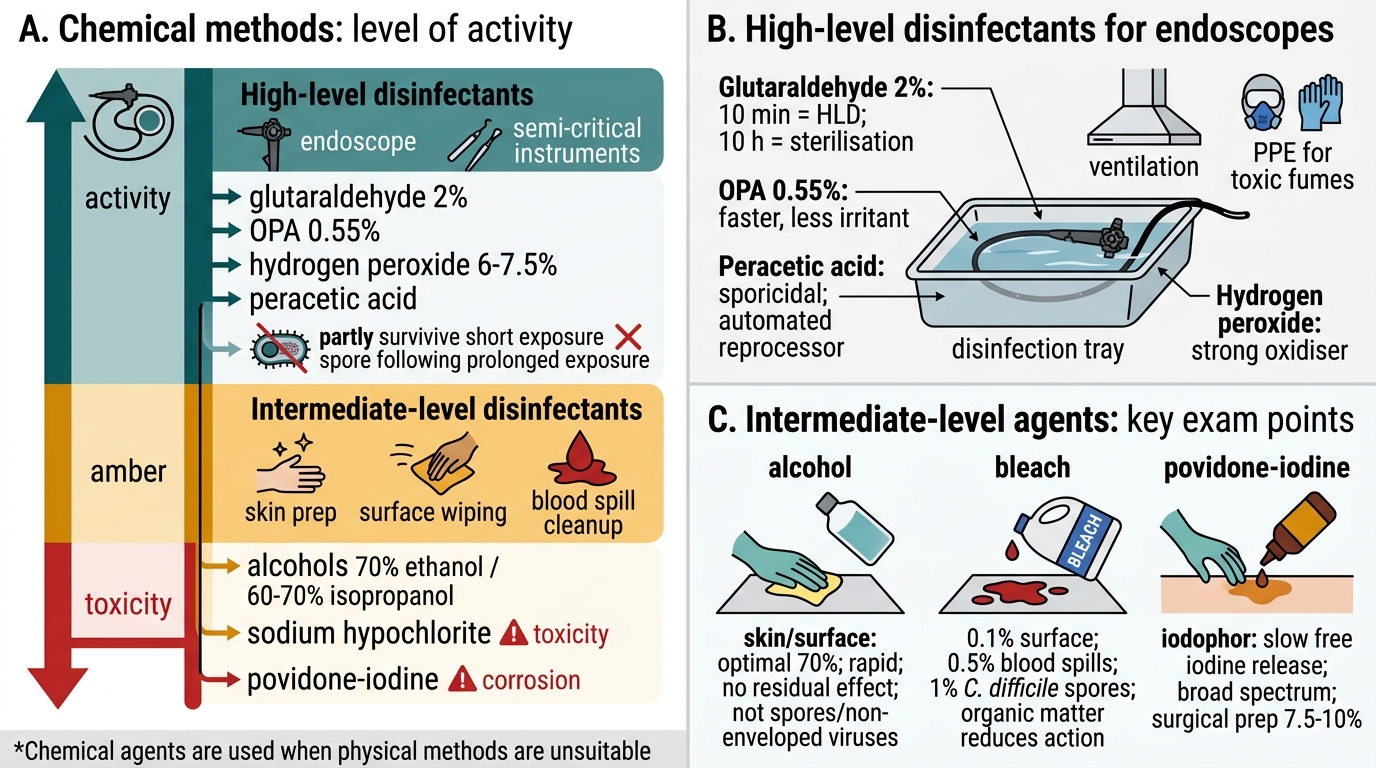
Chemical agents are used when physical methods are unsuitable. They are classified by level of activity:
High-level disinfectants (HLD) — kill all organisms except some bacterial spores with prolonged exposure:
• Glutaraldehyde (2%): gold standard HLD for endoscopes; effective at 20-25°C; 10-min exposure = HLD, 10-hour exposure = sterilisation. Toxic fumes — use in ventilated areas; personal protective equipment required.
• Ortho-phthalaldehyde (OPA, 0.55%): faster acting than glutaraldehyde, less irritant, used for endoscopes.
• Hydrogen peroxide (6-7.5%): strong oxidiser; used for surface disinfection and semi-critical items.
• Peracetic acid: sporicidal at low concentrations; used in automated endoscope reprocessors.
Intermediate-level disinfectants:
• Alcohols (70% ethanol, 60-70% isopropanol): denature proteins, disrupt lipid membranes. Rapid action; no residual effect. Used for skin antisepsis, surface disinfection. NOT effective against non-enveloped viruses (Norovirus) or spores. Optimal at 70% (water needed for denaturation).
• Sodium hypochlorite (bleach): 0.1% (1000 ppm) for general surface disinfection; 0.5% (5000 ppm) for blood spills; 1% for C. difficile contamination (spores). Strong oxidiser; corrosive to metals; inactivated by organic matter.
• Iodophors (Povidone-iodine): iodine complexed with polyvinylpyrrolidone (PVP); slow release of free iodine; broad spectrum; used for surgical skin prep (7.5-10% Betadine scrub), wound antisepsis.
• Phenol and phenolics: denature proteins, disrupt membranes; used for environmental disinfection. NOT for skin (caustic).
Low-level disinfectants:
• Quaternary ammonium compounds (QAC, e.g., benzalkonium chloride): disrupts Gram-positive bacteria membranes; fungicidal. INEFFECTIVE against Gram-negative bacilli, M. tuberculosis, non-enveloped viruses, spores. Used for routine surface cleaning.
• Chlorhexidine gluconate (0.5-4%): long-lasting skin antiseptic; effective against Gram-positives; moderate Gram-negative activity; used in surgical hand rubs, central line care, dental practice.

Chemical Disinfectants by Activity Level
Ethylene oxide (EtO) gas:
A chemical sterilant for heat-labile items (plastics, electronics, endoscopes, catheters). Mechanism: alkylates nucleic acids and proteins. Long aeration time needed (12-24 hr) to remove toxic residues. Used commercially for single-use device sterilisation. Carcinogenic — strictly regulated.
Choosing the Right Method — Clinical Decision Framework
Choosing the Right Sterilisation or Disinfection Method
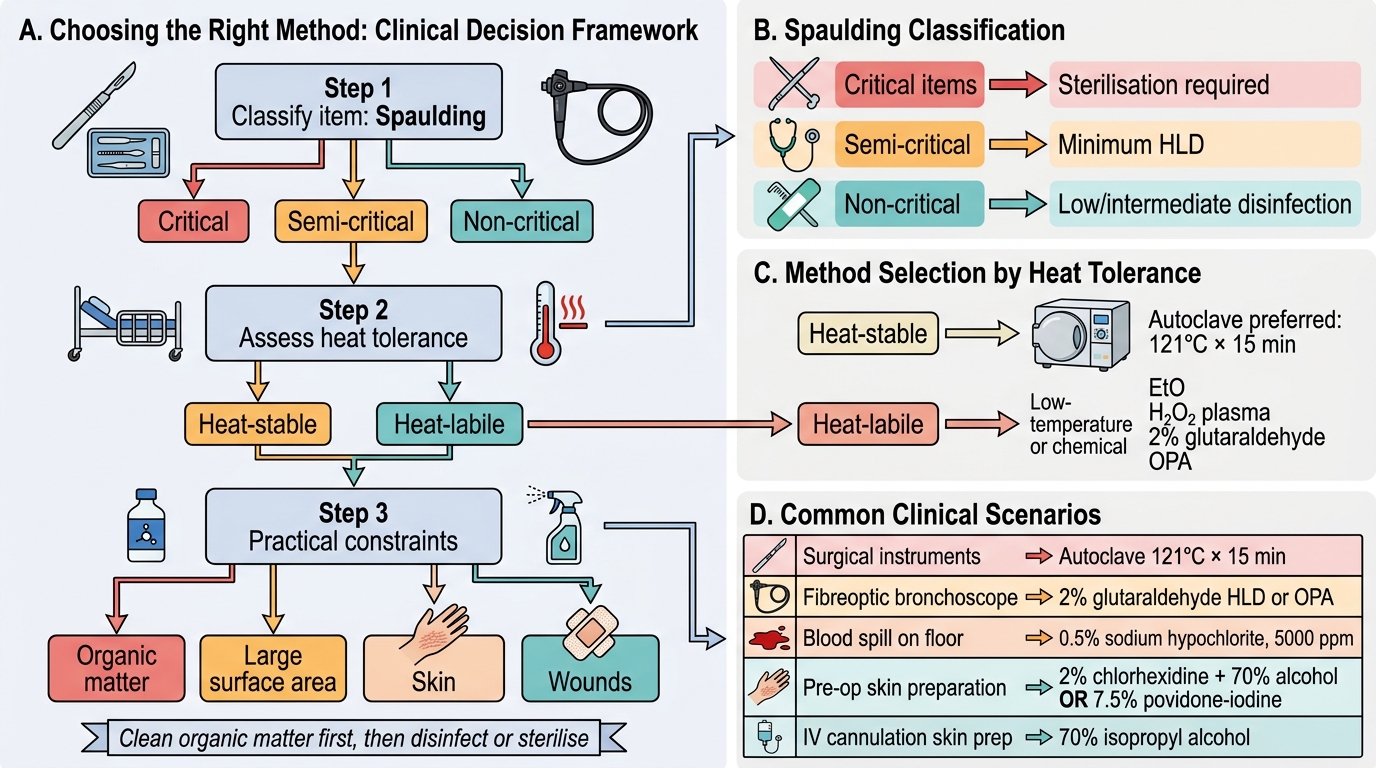
MI1.13 requires you to select the appropriate method for specific situations. Use this systematic approach:
Step 1 — Classify the item (Spaulding):
• Critical → sterilisation required
• Semi-critical → minimum HLD
• Non-critical → low/intermediate disinfection
Step 2 — Assess heat tolerance:
• Heat-stable → autoclave (preferred, most reliable, cheapest)
• Heat-labile → chemical or low-temperature physical (EtO, H₂O₂ plasma, glutaraldehyde)
Step 3 — Consider practical constraints:
• Organic matter present? → clean first, then disinfect/sterilise
• Large surface area? → fumigation, sodium hypochlorite spray
• Skin? → antiseptic only (never sterilants)
• Wounds? → aqueous povidone-iodine, dilute sodium hypochlorite (Dakin's)
Common clinical scenarios:
| Situation | Correct choice |
|---|---|
| Surgical instruments (SS) | Autoclave 121°C ×15 min |
| Fibreoptic bronchoscope | 2% glutaraldehyde (HLD) or OPA |
| Blood spill on floor | 0.5% sodium hypochlorite (5000 ppm) |
| Pre-op skin preparation | 2% chlorhexidine + 70% alcohol OR 7.5% povidone-iodine |
| IV cannulation skin prep | 70% isopropyl alcohol (swab, 30-sec contact) |
| C. difficile contaminated area | 1% sodium hypochlorite (10,000 ppm); alcohol INEFFECTIVE |
| Heat-sensitive electronic endoscope | Ethylene oxide or H₂O₂ gas plasma |
| Culture media preparation | Autoclave |
| Serum/antibiotic solution | Membrane filtration (0.22 µm) |
| OT air supply | HEPA filtration |
| Dental handpieces | Autoclave (134°C × 3 min, pre-vacuum) |
SELF-CHECK
A patient with Clostridioides difficile diarrhoea has been nursed in a single room. At discharge, which agent should be used to decontaminate the environment?
A. 70% isopropyl alcohol wipes
B. Quaternary ammonium compound spray
C. Sodium hypochlorite 0.1% (1000 ppm)
D. Sodium hypochlorite 1% (10,000 ppm)
Reveal Answer
Answer: D. Sodium hypochlorite 1% (10,000 ppm)
C. difficile forms spores that are resistant to alcohol and quaternary ammonium compounds. Sodium hypochlorite at high concentration (10,000 ppm = 1%) is sporicidal and is the agent of choice for C. difficile environmental decontamination. The lower concentration (1000 ppm) is used for routine surface disinfection and is insufficient for spore elimination.
REFLECT
You are working as a house officer in a surgical unit. The scrub nurse informs you that the autoclave indicator tape on today's instrument set changed colour but the biological indicator (Geobacillus strip) from last week's cycle grew on incubation — meaning the autoclave may have been malfunctioning. The instruments have already been used. What would you do? Consider: what information do you need, who do you inform, what are the implications for the patients operated upon last week, and how does this inform the quality control process going forward? This is a real-world sterilisation failure scenario.
KEY TAKEAWAYS
Sterilisation destroys all microorganisms including spores; disinfection eliminates most pathogens from inanimate surfaces; antisepsis applies to living tissue.
Spaulding classification drives the choice: critical items → sterilise; semi-critical → HLD minimum; non-critical → low/intermediate disinfection.
Physical methods:
• Autoclave (121°C/15 psi/15 min) — gold standard for heat-stable items; QC via biological indicators (G. stearothermophilus)
• Hot air oven — for glassware, oily materials
• Filtration (0.22 µm) — for heat-labile liquids
• Radiation — ionising (industrial sterilisation), UV (surface decontamination only)
Chemical methods:
• High-level: glutaraldehyde 2%, OPA — endoscopes
• Intermediate: 70% alcohol (skin), sodium hypochlorite (surfaces, blood spills)
• Low-level: QAC, chlorhexidine (skin antisepsis)
• Chemical sterilant: ethylene oxide (heat-labile items)
C. difficile exception: alcohol is ineffective; use high-concentration hypochlorite (10,000 ppm).